

Tibial lengthening: extraarticular calcaneotibial screw to prevent ankle equinus
- PMID: 18800215
- PMCID: PMC2628241
- DOI: 10.1007/s11999-008-0489-8
Tibial lengthening: extraarticular calcaneotibial screw to prevent ankle equinus
Abstract
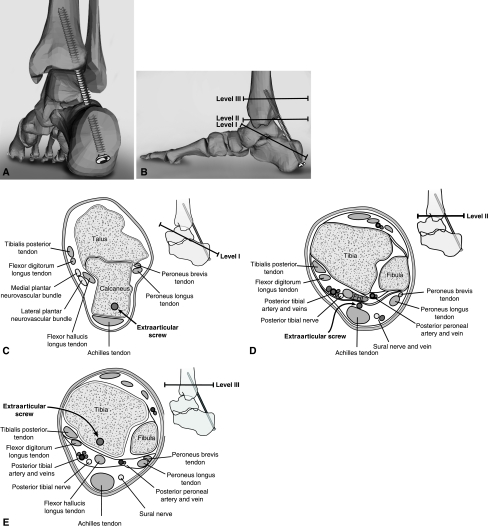
Between 2003 and 2006, we used an extraarticular, cannulated, fully threaded posterior calcaneotibial screw to prevent equinus contracture in 10 patients (four male and six female patients, 14 limbs) undergoing tibial lengthening with the intramedullary skeletal kinetic distractor. Diagnoses were fibular hemimelia (two), mesomelic dwarfism (two), posteromedial bow (one), hemihypertrophy (one), poliomyelitis (one), achondroplasia (one), posttraumatic limb-length discrepancy (one), and hypochondroplasia (one). Average age was 24.5 years (range, 15-54 years). The screw (length, typically 125 mm; diameter, 7 mm) was inserted with the ankle in 10 degrees dorsiflexion. Gastrocnemius soleus recession was performed in two patients to achieve 10 degrees dorsiflexion. Average lengthening was 4.9 cm (range, 3-7 cm). Screws were removed after a mean 3.3 months (range, 2-6 months). Preoperative ankle range of motion was regained within 6 months of screw removal. No neurovascular complications were encountered, and no patients experienced equinus contracture. We also conducted a cadaveric study in which one surgeon inserted screws in eight cadaveric legs under image intensifier control. The flexor hallucis longus muscle belly was the closest anatomic structure noted during dissection. The screw should be inserted obliquely from upper lateral edge of the calcaneus and aimed lateral in the tibia to avoid the flexor hallucis longus muscle.
Level of evidence: Level IV, therapeutic study. See the Guidelines for Authors for a complete description of levels of evidence.
Figures



References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '535265', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/535265/'}]}
- Ahmadi B, Akbarnia BA, Ghobadi F, Ganjavian MS, Nasseri D. Experience with 141 tibial lengthenings in poliomyelitis and comparison of 3 different methods. Clin Orthop Relat Res. 1979;145:150–153. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '10360691', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/10360691/'}]}
- Aldegheri R. Distraction osteogenesis for lengthening of the tibia in patients who have limb-length discrepancy or short stature. J Bone Joint Surg Am. 1999;81:624–634. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1097/00003086-199710000-00023', 'is_inner': False, 'url': 'https://doi.org/10.1097/00003086-199710000-00023'}, {'type': 'PubMed', 'value': '9345218', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/9345218/'}]}
- Baumgart R, Betz A, Schweiberer L. A fully implantable motorized intramedullary nail for limb lengthening and bone transport. Clin Orthop Relat Res. 1997;343:135–143. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1016/S0002-9610(29)90110-0', 'is_inner': False, 'url': 'https://doi.org/10.1016/s0002-9610(29)90110-0'}]}
- Campbell WC. An operation for the induction of osseous fusion in the ankle joint. Am J Surg. 1929;6:588.
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1016/S0020-1383(01)00116-4', 'is_inner': False, 'url': 'https://doi.org/10.1016/s0020-1383(01)00116-4'}, {'type': 'PubMed', 'value': '11812486', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/11812486/'}]}
- Cole JD, Justin D, Kasparis T, DeVlught D, Knobloch C. The intramedullary skeletal kinetic distractor (ISKD): first clinical results of a new intramedullary nail for lengthening of the femur and tibia. Injury. 2001;32(Suppl 4):SD129–SD139. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
