

An integrated system for planning, navigation and robotic assistance for skull base surgery
- PMID: 18803337
- PMCID: PMC2770335
- DOI: 10.1002/rcs.213
An integrated system for planning, navigation and robotic assistance for skull base surgery
Abstract
Background: We developed an image-guided robot system to provide mechanical assistance for skull base drilling, which is performed to gain access for some neurosurgical interventions, such as tumour resection. The motivation for introducing this robot was to improve safety by preventing the surgeon from accidentally damaging critical neurovascular structures during the drilling procedure.
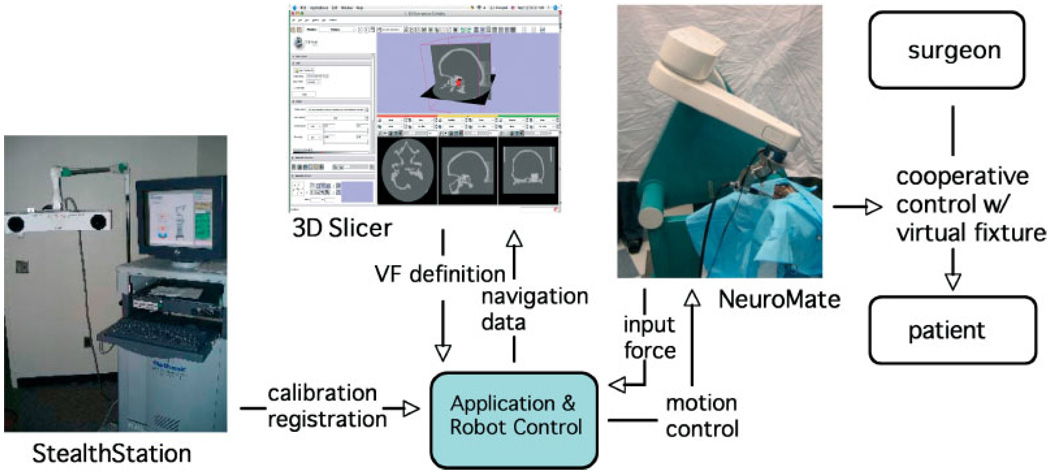
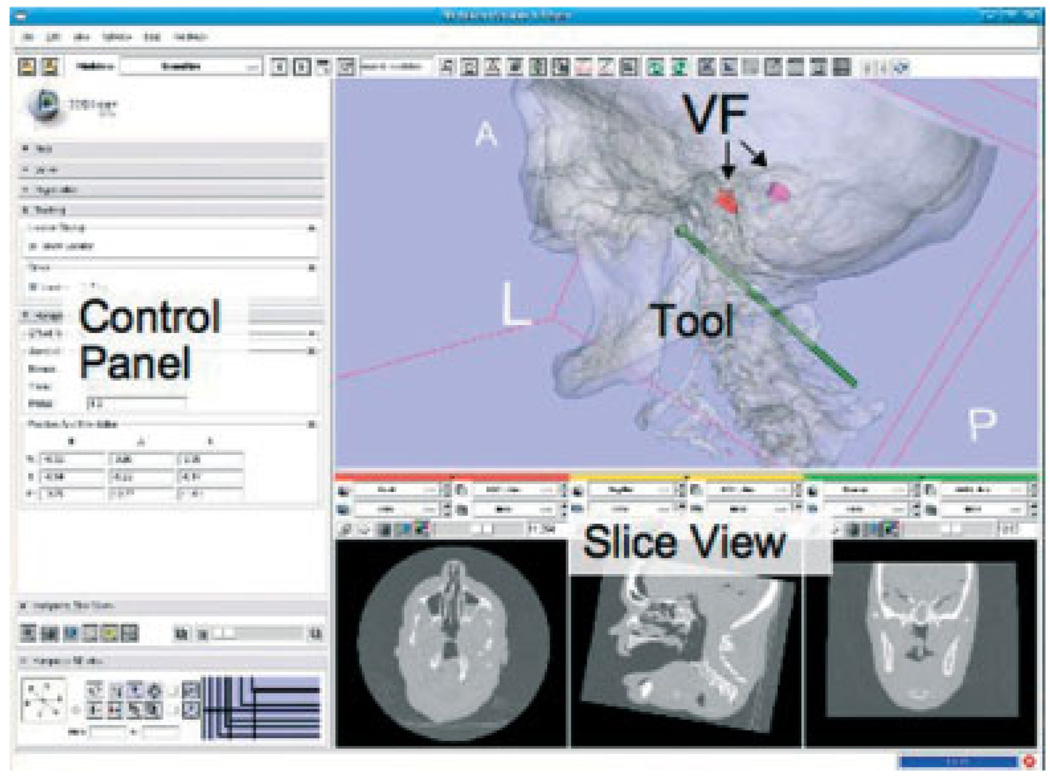
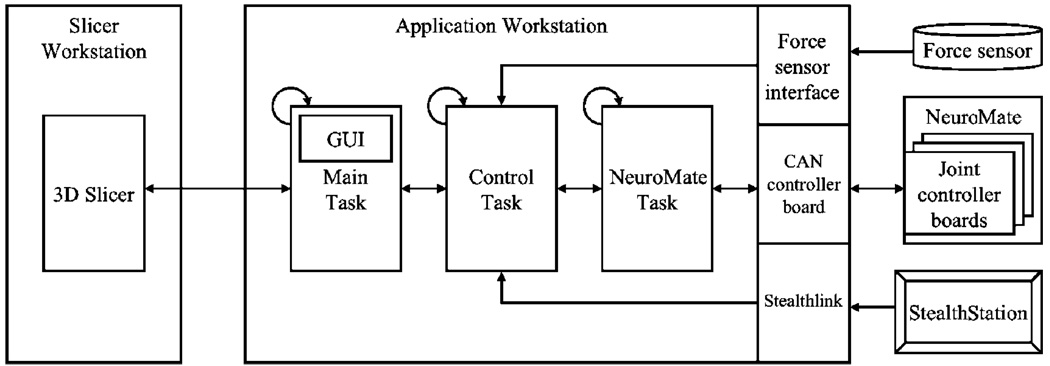
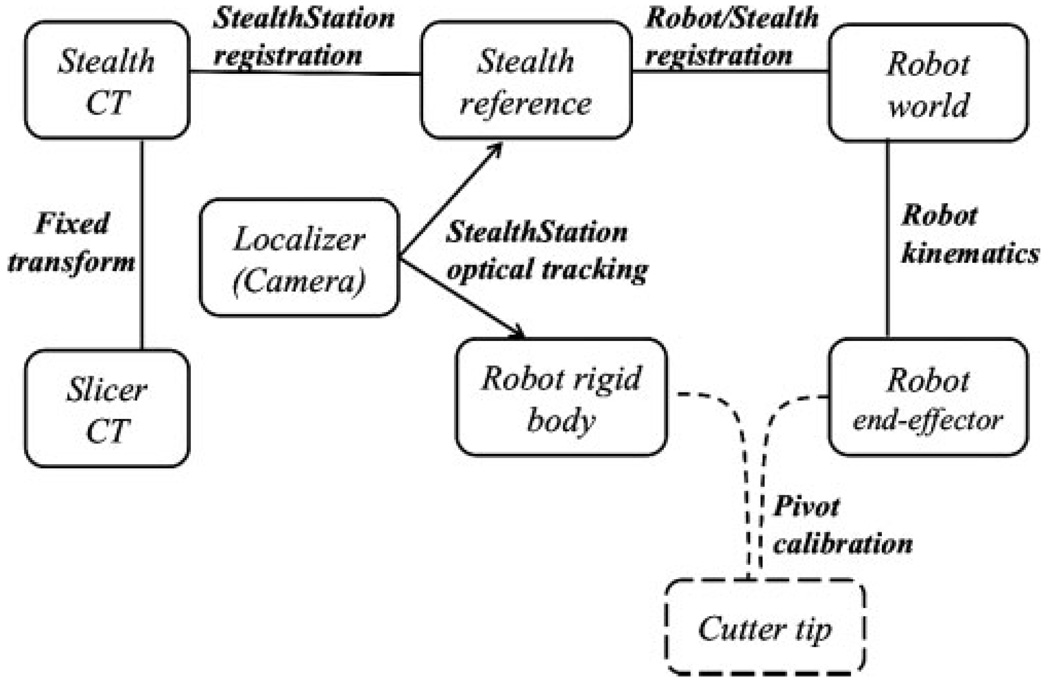
Methods: We integrated a Stealthstation navigation system, a NeuroMate robotic arm with a six-degree-of-freedom force sensor, and the 3D Slicer visualization software to allow the robotic arm to be used in a navigated, cooperatively-controlled fashion by the surgeon. We employed virtual fixtures to constrain the motion of the robot-held cutting tool, so that it remained in the safe zone that was defined on a preoperative CT scan.
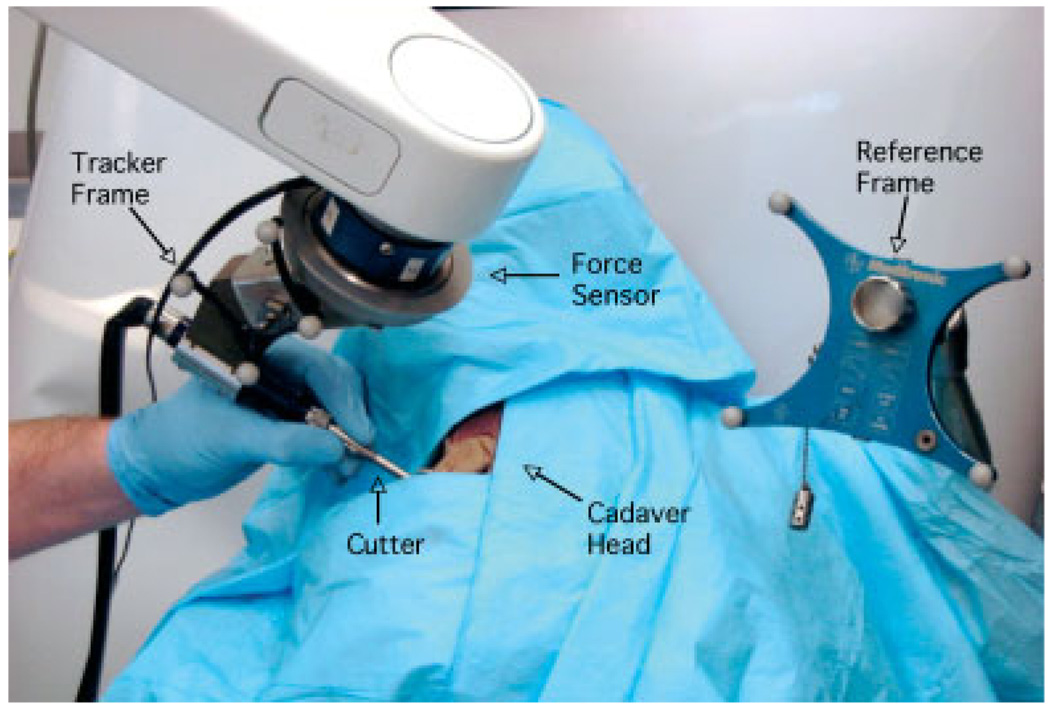
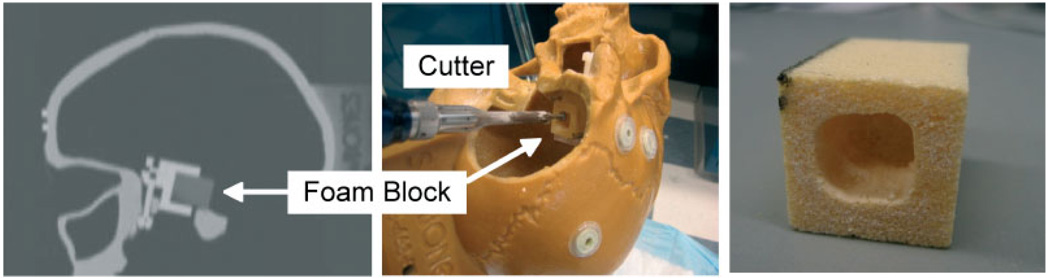
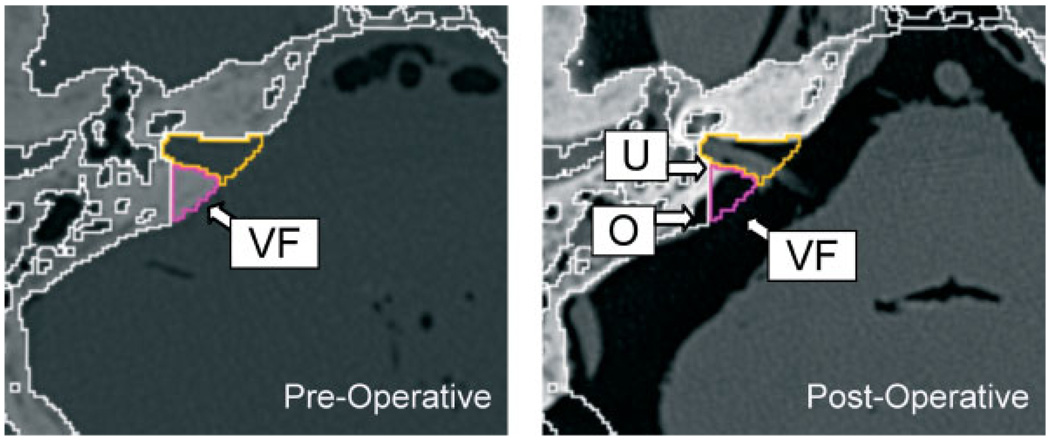
Results: We performed experiments on both foam skull and cadaver heads. The results for foam blocks cut using different registrations yielded an average placement error of 0.6 mm and an average dimensional error of 0.6 mm. We drilled the posterior porus acusticus in three cadaver heads and concluded that the robot-assisted procedure is clinically feasible and provides some ergonomic benefits, such as stabilizing the drill. We obtained postoperative CT scans of the cadaver heads to assess the accuracy and found that some bone outside the virtual fixture boundary was cut. The typical overcut was 1-2 mm, with a maximum overcut of about 3 mm.
Conclusions: The image-guided cooperatively-controlled robot system can improve the safety and ergonomics of skull base drilling by stabilizing the drill and enforcing virtual fixtures to protect critical neurovascular structures. The next step is to improve the accuracy so that the overcut can be reduced to a more clinically acceptable value of about 1 mm.
Figures

Similar articles
-
A cooperatively-controlled image guided robot system for skull base surgery.Stud Health Technol Inform. 2008;132:198-203. Stud Health Technol Inform. 2008. PMID: 18391286
-
Distance Control and Virtual Drilling Improves Anatomical Orientation During Anterior Petrosectomy.Oper Neurosurg. 2020 Jan 1;18(1):83-91. doi: 10.1093/ons/opz064. Oper Neurosurg. 2020. PMID: 31323686 Free PMC article.
-
An automated robotic approach with redundant navigation for minimal invasive extended transsphenoidal skull base surgery.Minim Invasive Neurosurg. 2005 Jun;48(3):159-64. doi: 10.1055/s-2005-870903. Minim Invasive Neurosurg. 2005. PMID: 16015493
-
[Surgical robotics in neurosurgery].Orv Hetil. 2009 Sep 6;150(36):1701-11. doi: 10.1556/OH.2009.28701. Orv Hetil. 2009. PMID: 19709985 Review. Hungarian.
-
Robotic and robot-assisted skull base neurosurgery: systematic review of current applications and future directions.Neurosurg Focus. 2022 Jan;52(1):E15. doi: 10.3171/2021.10.FOCUS21505. Neurosurg Focus. 2022. PMID: 34973668
Cited by
-
Three-dimensional printing and 3D slicer powerful tools in understanding and treating neurosurgical diseases.Front Surg. 2022 Oct 14;9:1030081. doi: 10.3389/fsurg.2022.1030081. eCollection 2022. Front Surg. 2022. PMID: 36311943 Free PMC article. Review.
-
Robotic hypospadias surgery: a new evolution.J Robot Surg. 2010 Jan;3(4):239-44. doi: 10.1007/s11701-009-0165-3. Epub 2009 Nov 26. J Robot Surg. 2010. PMID: 27628637
-
A Cooperatively Controlled Robot for Ultrasound Monitoring of Radiation Therapy.Rep U S. 2013 Nov;2013:3071-3076. doi: 10.1109/IROS.2013.6696791. Rep U S. 2013. PMID: 26823988 Free PMC article.
-
Determination of the curling behavior of a preformed cochlear implant electrode array.Int J Comput Assist Radiol Surg. 2011 May;6(3):421-33. doi: 10.1007/s11548-010-0520-x. Epub 2010 Jul 28. Int J Comput Assist Radiol Surg. 2011. PMID: 20665247
-
Installation of a Neuromate Robot for Stereotactic Surgery: Efforts to Conform to Japanese Specifications and an Approach for Clinical Use-Technical Notes.Neurol Med Chir (Tokyo). 2015;55(12):907-14. doi: 10.2176/nmc.tn.2015-0043. Epub 2015 Oct 28. Neurol Med Chir (Tokyo). 2015. PMID: 26511113 Free PMC article.
References
-
- Matinfar M, Baird C, Batouli A, et al. Robot assisted skull base surgery; IEEE International Conference on Intelligent Robots and Systems; 2007. pp. 865–870.
-
- Jakopec M, Rodriguez y, Baena F, Harris SJ, et al. The hands-on orthopaedic robot ‘Acrobot’: early clinical trials of total knee replacement surgery. IEEE Trans Robotics Autom. 2003;19(5):902–911.
-
- Li M, Ishii M, Taylor RH. Spatialmotion constraints using virtual fixtures generated by anatomy. IEEE Trans Robotics. 2007;23(1):4–19.
-
- Sim C, Ng WS, Teo MY, et al. Image guided manipulator compliant surgical planning methodology for robotic skull-base surgery. Intertnational Workshop on Medical Imaging and Augmented Reality; June 2001; Hong Kong, China. pp. 26–29.
-
- Bumm K, Wurm J, Rachinger J, et al. An automated robotic approach with redundant navigation for minimal invasive extended transsphenoidal skull base surgery. Minim Invas Neurosurg. 2005;48(3):159–164. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
