

Post tracheostomy and post intubation tracheal stenosis: report of 31 cases and review of the literature
- PMID: 18803874
- PMCID: PMC2556644
- DOI: 10.1186/1471-2466-8-18
Post tracheostomy and post intubation tracheal stenosis: report of 31 cases and review of the literature
Abstract
Background: Severe post tracheostomy (PT) and post intubation (PI) tracheal stenosis is an uncommon clinical entity that often requires interventional bronchoscopy before surgery is considered. We present our experience with severe PI and PT stenosis in regards to patient characteristics, possible risk factors, and therapy.
Methods: We conducted a retrospective chart review of 31 patients with PI and PT stenosis treated at Lahey Clinic over the past 8 years. Demographic characteristics, body mass index, co-morbidities, stenosis type and site, procedures performed and local treatments applied were recorded.
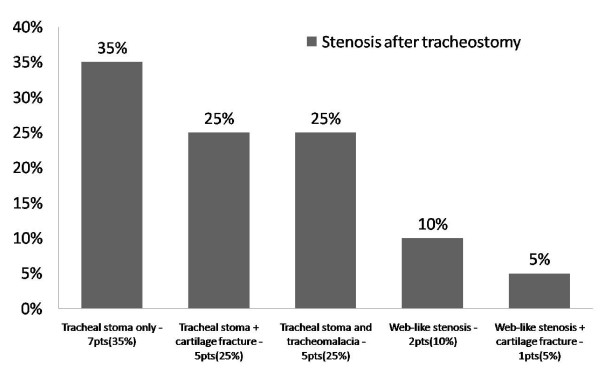
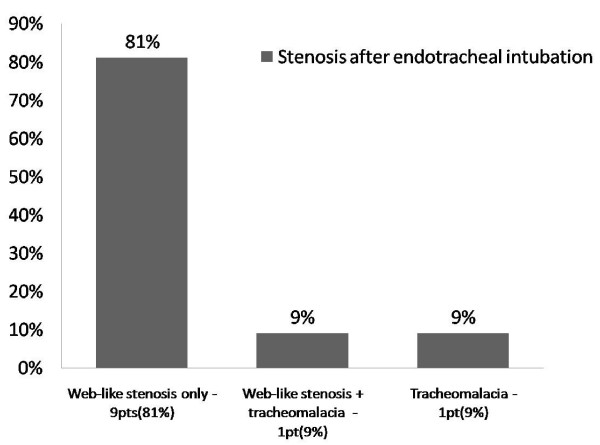
Results: The most common profile of a patient with tracheal stenosis in our series was a female (75%), obese (66%) patient with a history of diabetes mellitus (35.4%), hypertension (51.6%), and cardiovascular disease (45.1%), who was a current smoker (38.7%). Eleven patients (PI group) had only oro-tracheal intubation (5.2 days of intubation) and developed web-like stenosis at the cuff site. Twenty patients (PT group) had undergone tracheostomy (54.5 days of intubation) and in 17 (85%) of them the stenosis appeared around the tracheal stoma. There was an average of 2.4 procedures performed per patient. Rigid bronchoscopy with Nd:YAG laser and dilatation (mechanical or balloon) were the preferred methods used. Only 1(3.2%) patient was sent to surgery for re-stenosis after multiple interventional bronchoscopy treatments.
Conclusion: We have identified putative risk factors for the development of PI and PT stenosis. Differences in lesions characteristics and stenosis site were noted in our two patient groups. All patients underwent interventional bronchoscopy procedures as the first-line, and frequently the only treatment approach.
Figures
References
-
- Kastanos N, Estopa Miro R, Marin Perez A, Xaubet Mir A, Agusti-Vidal A. Laryngotracheal injury due to endotracheal intubation: incidence, evolution, and predisposing factors. A prospective long-term study. Critical care medicine. 1983;11:362–367. doi: 10.1097/00003246-198305000-00009. - DOI - PubMed
-
- Pearson FG, Andrews MJ. Detection and management of tracheal stenosis following cuffed tube tracheostomy. The Annals of thoracic surgery. 1971;12:359–374. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
