

Predictors of outcome for short-term medically supervised opioid withdrawal during a randomized, multicenter trial of buprenorphine-naloxone and clonidine in the NIDA clinical trials network drug and alcohol dependence
- PMID: 18805656
- PMCID: PMC2770269
- DOI: 10.1016/j.drugalcdep.2008.06.016
Predictors of outcome for short-term medically supervised opioid withdrawal during a randomized, multicenter trial of buprenorphine-naloxone and clonidine in the NIDA clinical trials network drug and alcohol dependence
Abstract
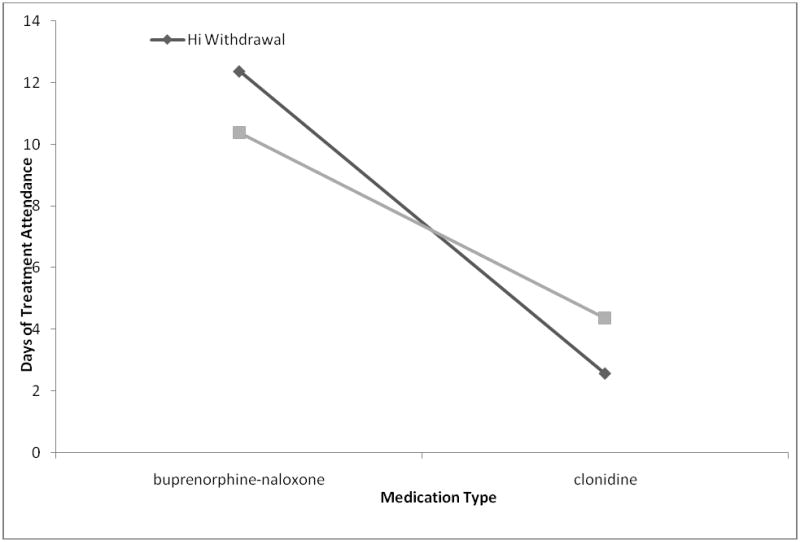
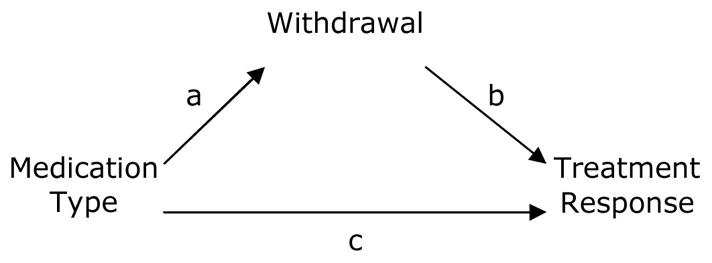
Few studies in community settings have evaluated predictors, mediators, and moderators of treatment success for medically supervised opioid withdrawal treatment. This report presents new findings about these factors from a study of 344 opioid-dependent men and women prospectively randomized to either buprenorphine-naloxone or clonidine in an open-label 13-day medically supervised withdrawal study. Subjects were either inpatient or outpatient in community treatment settings; however not randomized by treatment setting. Medication type (buprenorphine-naloxone versus clonidine) was the single best predictor of treatment retention and treatment success, regardless of treatment setting. Compared to the outpatient setting, the inpatient setting was associated with higher abstinence rates but similar retention rates when adjusting for medication type. Early opioid withdrawal severity mediated the relationship between medication type and treatment outcome with buprenorphine-naloxone being superior to clonidine at relieving early withdrawal symptoms. Inpatient subjects on clonidine with lower withdrawal scores at baseline did better than those with higher withdrawal scores; inpatient subjects receiving buprenorphine-naloxone did better with higher withdrawal scores at baseline than those with lower withdrawal scores. No relationship was found between treatment outcome and age, gender, race, education, employment, marital status, legal problems, baseline depression, or length/severity of drug use. Tobacco use was associated with worse opioid treatment outcomes. Severe baseline anxiety symptoms doubled treatment success. Medication type (buprenorphine-naloxone) was the most important predictor of positive outcome; however the paper also considers other clinical and policy implications of other results, including that inpatient setting predicted better outcomes and moderated medication outcomes.
Conflict of interest statement
D.M.Z. has consulted for Pfizer, Bristol-Myers Squibb, Janssen, Eli Lilly, and Alkermes/Cephalon. D.M.Z. has received grant support from Bristol-Myers Squibb, Janssen, and Eli Lilly. L.A. is currently employed by Schering-Plough, a distributor of buprenorphine. G.W. has consulted for Denver Health. S.M.S. has received grant support from Purdue Pharma, US WorldMeds LLC, and Titan Pharmaceuticals. L.A. and T.H. have received honoraria from Reckitt Benckiser and Schering Plough.
All other authors declare they have no conflicts of interest.
Figures
References
-
- Araujo L, Goldberg P, Eyma J, et al. The effect of anxiety and depression on completion and withdrawal status in patients admitted to substance abuse detoxification program. Journal of Substance Abuse Treatment. 1996;13:61–66. - PubMed
-
- Amass L, Kamien JB, Mikulich SK. Efficacy of daily and alternate-day dosing regimens with the combination buprenorphine-naloxone tablet. Drug Alcohol Depend. 2000;58(1–2):143–52. - PubMed
-
- American Psychiatric Association. Practice Guidelines for the Treatment of Patients With Substance Use Disorders. American Psychiatric Press Inc; Washington DC: 2006.
-
- Armenia SH, Chutuape MA, Stitzer ML. Predictors of discharge against medical advice from a short-term hospital detoxification unit. Drug Alcohol Depend. 1999;56(1):1–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U10 DA013046/DA/NIDA NIH HHS/United States
- U10 DA13046/DA/NIDA NIH HHS/United States
- M01RR00096/RR/NCRR NIH HHS/United States
- U10 DA013710/DA/NIDA NIH HHS/United States
- U10 DA13720/DA/NIDA NIH HHS/United States
- U10 DA013045/DA/NIDA NIH HHS/United States
- U10 DA13710/DA/NIDA NIH HHS/United States
- U10 DA013720/DA/NIDA NIH HHS/United States
- U10 DA13045/DA/NIDA NIH HHS/United States
- U10 DA013035/DA/NIDA NIH HHS/United States
- M01 RR000096/RR/NCRR NIH HHS/United States
- K05 DA017009/DA/NIDA NIH HHS/United States
- U10 DA13043/DA/NIDA NIH HHS/United States
- U10 DA013036/DA/NIDA NIH HHS/United States
- U10 DA013732/DA/NIDA NIH HHS/United States
- U10 DA013043/DA/NIDA NIH HHS/United States
- U10 DA13732/DA/NIDA NIH HHS/United States
- U10DA13036/DA/NIDA NIH HHS/United States
- U10 DA13035/DA/NIDA NIH HHS/United States
- K05 DA-17009/DA/NIDA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
