

Dependence of hearing changes on the dose of intratympanically applied gentamicin: a meta-analysis using mathematical simulations of clinical drug delivery protocols
- PMID: 18806480
- PMCID: PMC2741178
- DOI: 10.1097/MLG.0b013e31817d01cd
Dependence of hearing changes on the dose of intratympanically applied gentamicin: a meta-analysis using mathematical simulations of clinical drug delivery protocols
Abstract
Objectives/hypothesis: To establish safe dosing protocols for the treatment of patients with Meniere's disease with intratympanic gentamicin.
Study design: A validated computer model of gentamicin dispersion in the inner ear fluids was used to calculate cochlear drug levels resulting from specific clinical delivery protocols. Dosing in the cochlea was compared with changes of hearing sensitivity for 568 patients reported in 19 publications.
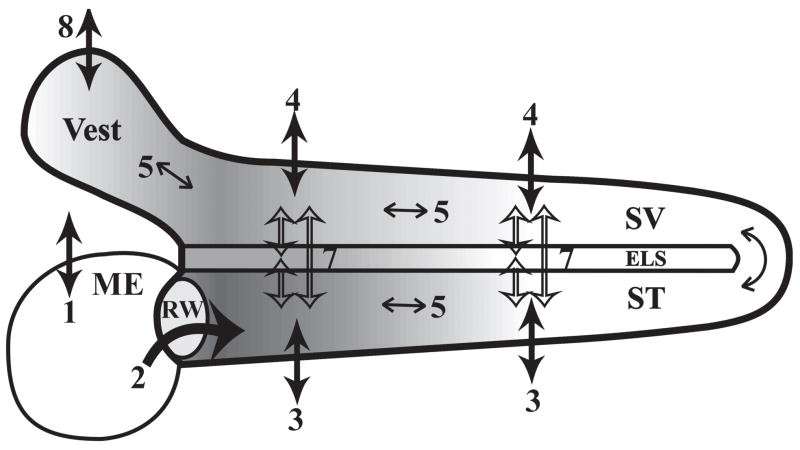
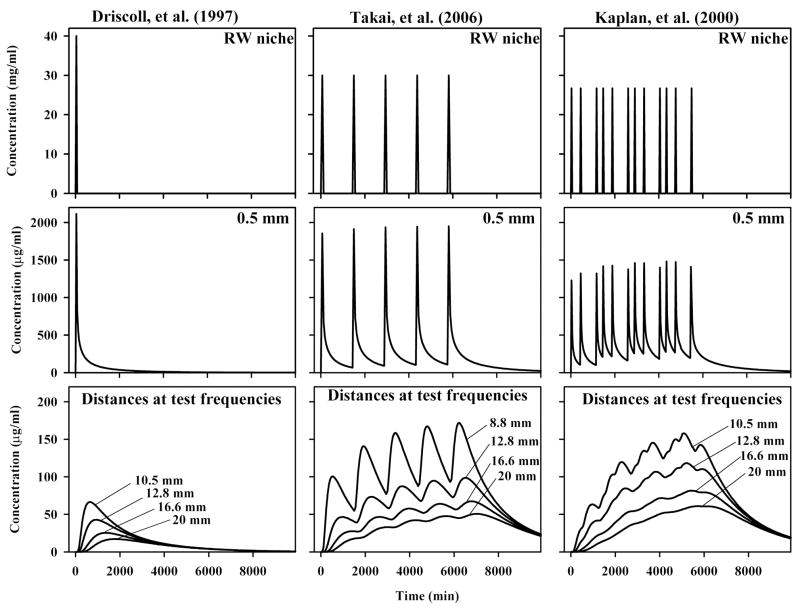
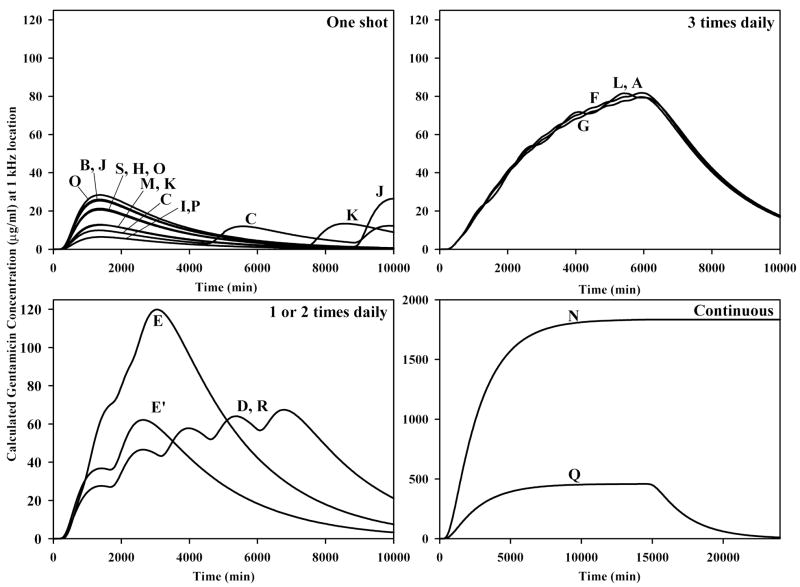
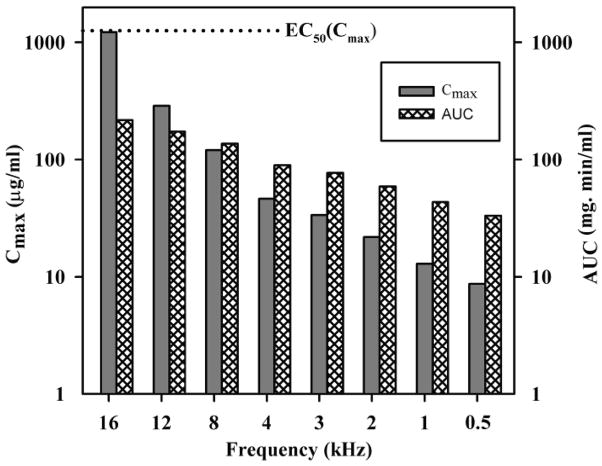
Methods: Cochlear drug levels were calculated based on the concentration and volume of gentamicin applied, the time the drug remained in the middle ear, and on the specific timing of injections. Time courses were quantified in terms of the maximum concentration (Cmax) and the area under the curve of the drug at specific cochlear locations.
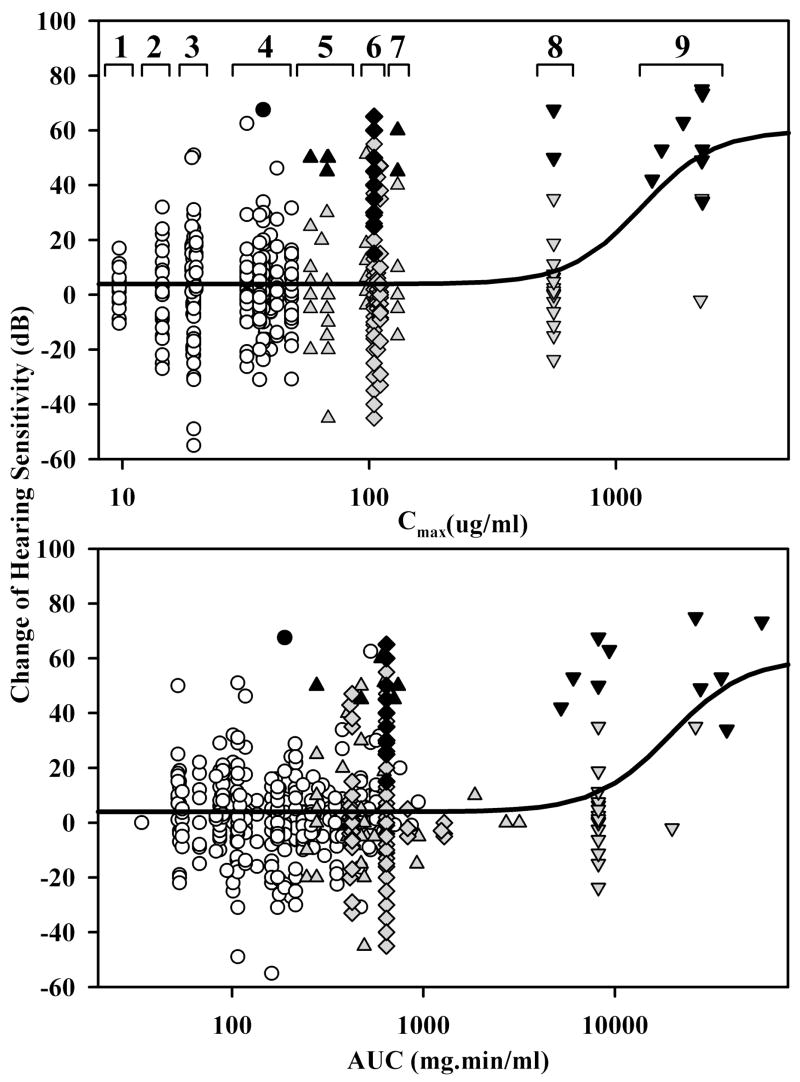
Results: Drug levels resulting from single, "one-shot" injections were typically lower than those from repeated or continuous application protocols. Comparison of hearing sensitivity changes with gentamicin dosing revealed a flat curve with a near-zero mean for lower doses, suggesting that hearing changes with doses over this range were probably unrelated to the applied drug. Higher intracochlear doses were generated with repeated or continuous delivery protocols, which in some cases caused substantial hearing losses and an increased incidence of deafened ears.
Conclusions: One-shot application protocols produce gentamicin doses in the cochlea that have minimal risk to hearing at the frequencies tested. Repeated or continuous application protocols result in higher doses that in some cases damage hearing. The high variability of hearing changes, even with low gentamicin doses, calls into question the rationale for using individual hearing changes to titrate the applied dose.
Figures
References
-
- Lange G. The intratympanic treatment of Meniere’s disease with ototoxic antibiotics. A follow-up study of 55 cases. Laryngol Rhinol Otol. 1977;56:409–414. - PubMed
-
- Lange G. Gentamicin and other ototoxic antibiotics for the transtympanic treatment of Meniere’s disease. Arch Otorhinolaryngol. 1989;246:269–270. - PubMed
-
- Lange G. 27 years experiences with transtympanic aminoglycoside treatment of Meniere’s disease. Laryngorhinootologie. 1995;74:720–723. - PubMed
-
- Salt AN, Ma Y. Quantification of solute entry into cochlear perilymph through the round window membrane. Hear Res. 2001;154:88–97. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
