

Enhanced Na+/H+ exchange during ischemia and reperfusion impairs mitochondrial bioenergetics and myocardial function
- PMID: 18806604
- PMCID: PMC2659015
- DOI: 10.1097/FJC.0b013e3181831337
Enhanced Na+/H+ exchange during ischemia and reperfusion impairs mitochondrial bioenergetics and myocardial function
Abstract
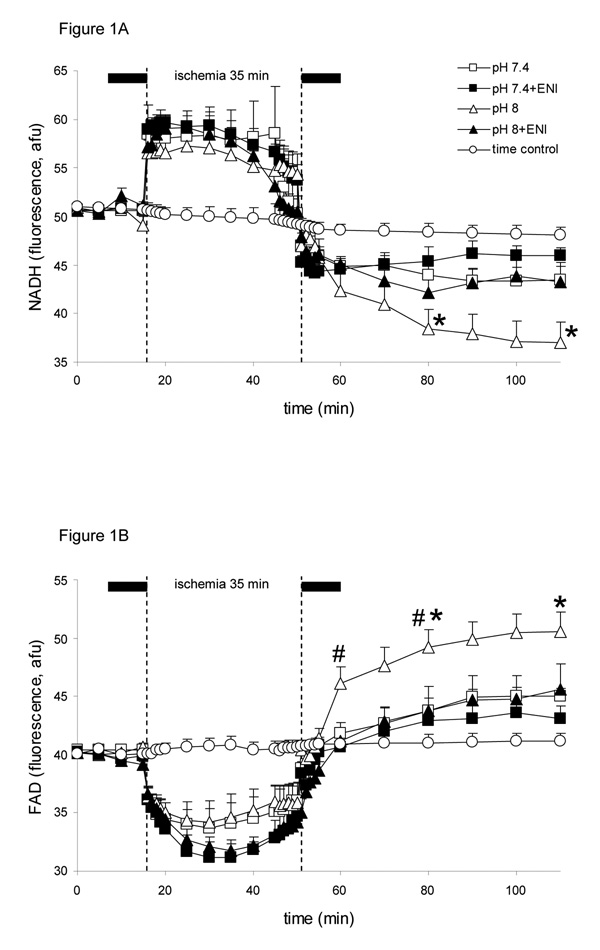
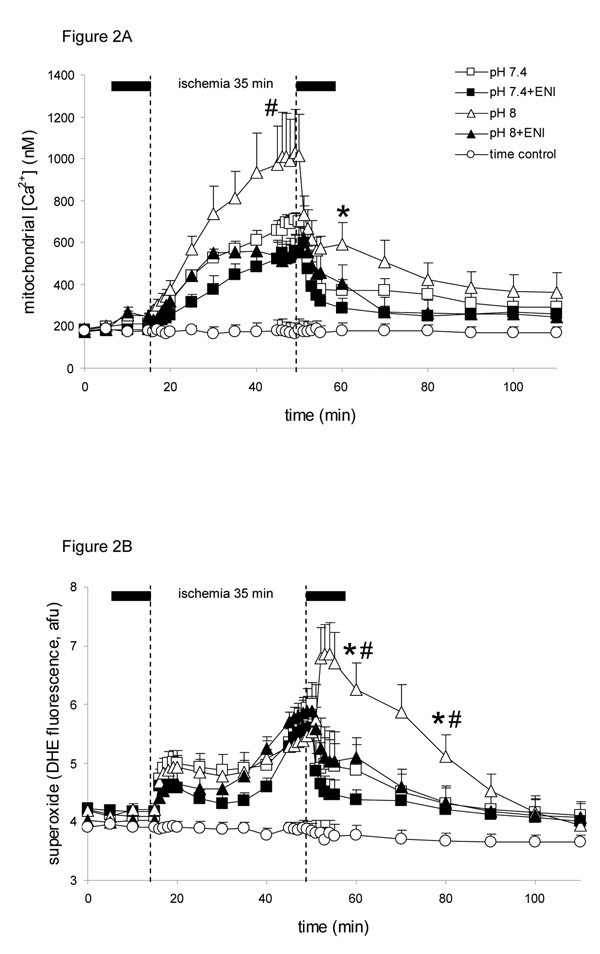
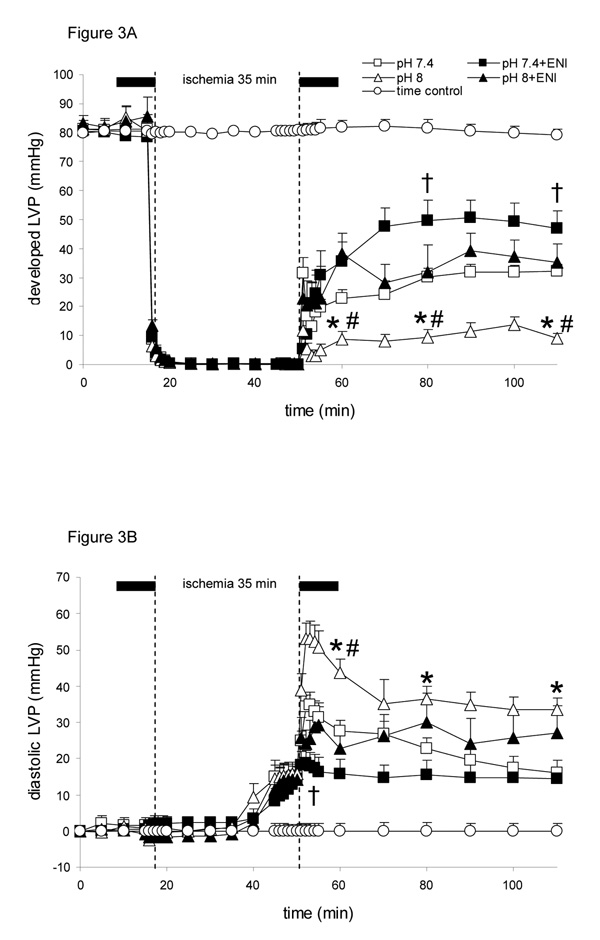
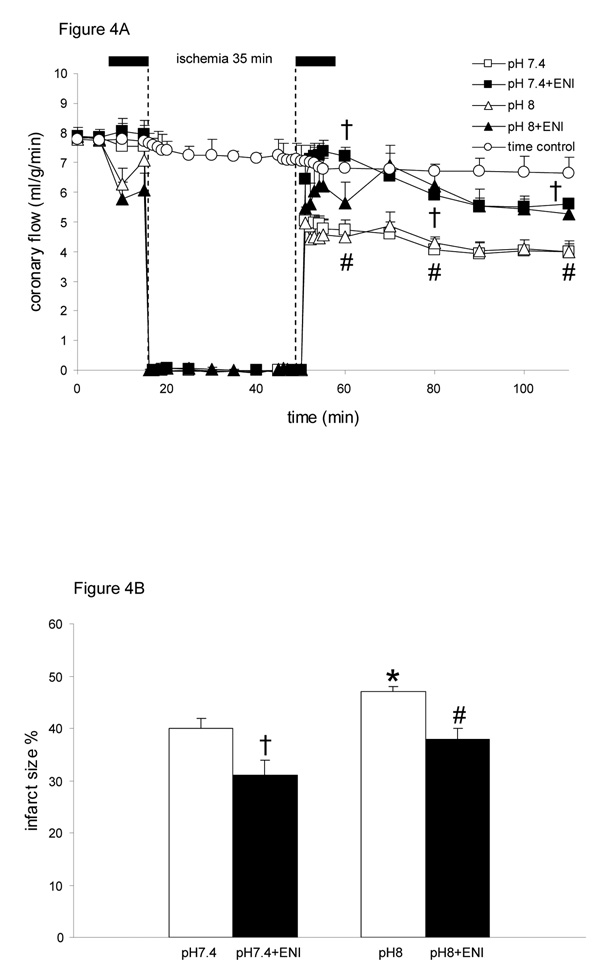
Inhibition of Na+/H+ exchange (NHE) during ischemia reduces cardiac injury due to reduced reverse mode Na+/Ca2+ exchange. We hypothesized that activating NHE-1 at buffer pH 8 during ischemia increases mitochondrial oxidation, Ca2+ overload, and reactive O2 species (ROS) levels and worsens functional recovery in isolated hearts and that NHE inhibition reverses these effects. Guinea pig hearts were perfused with buffer at pH 7.4 (control) or pH 8 +/- NHE inhibitor eniporide for 10 minutes before and for 10 minutes after 35- minute ischemia and then for 110 minutes with pH 7.4 buffer alone. Mitochondrial NADH and FAD, [Ca2+], and superoxide were measured by spectrophotofluorometry. NADH and FAD were more oxidized, and cardiac function was worse throughout reperfusion after pH 8 versus pH 7.4, Ca2+ overload was greater at 10-minute reperfusion, and superoxide generation was higher at 30-minute reperfusion. The pH 7.4 and eniporide groups exhibited similar mitochondrial function, and cardiac performance was most improved after pH 7.4+eniporide. Cardiac function on reperfusion after pH 8+eniporide was better than after pH 8. Percent infarction was largest after pH 8 and smallest after pH 7.4+eniporide. Activation of NHE with pH 8 buffer and the subsequent decline in redox state with greater ROS and Ca2+ loading underlie the poor functional recovery after ischemia and reperfusion.
Conflict of interest statement
Disclosures
The authors have no conflicts of interest to disclose.
Figures
References
-
- Brookes PS, Yoon Y, Robotham JL, et al. Calcium, ATP, and ROS: a mitochondrial love-hate triangle. Am J Physiol Cell Physiol. 2004;287:C817–C833. - PubMed
-
- Miyamae M, Camacho SA, Weiner MW, et al. Attenuation of postischemic reperfusion injury is related to prevention of [Ca2+]m overload in rat hearts. Am J Physiol. 1996;271:H2145–H2153. - PubMed
-
- Vaughan-Jones RD, Wu ML, Bountra C. Sodium-hydrogen exchange and its role in controlling contractility during acidosis in cardiac muscle. Mol Cell Biochem. 1989;89:157–162. - PubMed
-
- Karmazyn M. The role of the myocardial sodium-hydrogen exchanger in mediating ischemic and reperfusion injury. From amiloride to cariporide. Ann N Y Acad Sci. 1999;874:326–334. - PubMed
-
- Pike MM, Kitakaze M, Marban E. 23Na-NMR measurements of intracellular sodium in intact perfused ferret hearts during ischemia and reperfusion. Am J Physiol. 1990;259:H1767–H1773. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
