

Inhibition of lipoprotein-associated phospholipase A2 reduces complex coronary atherosclerotic plaque development
- PMID: 18806801
- PMCID: PMC2885134
- DOI: 10.1038/nm.1870
Inhibition of lipoprotein-associated phospholipase A2 reduces complex coronary atherosclerotic plaque development
Abstract
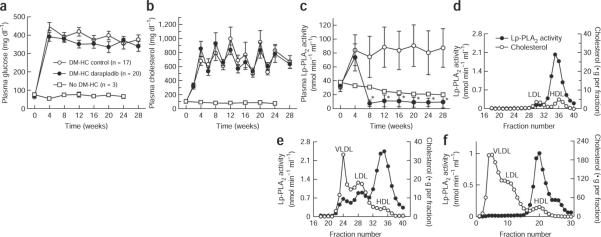
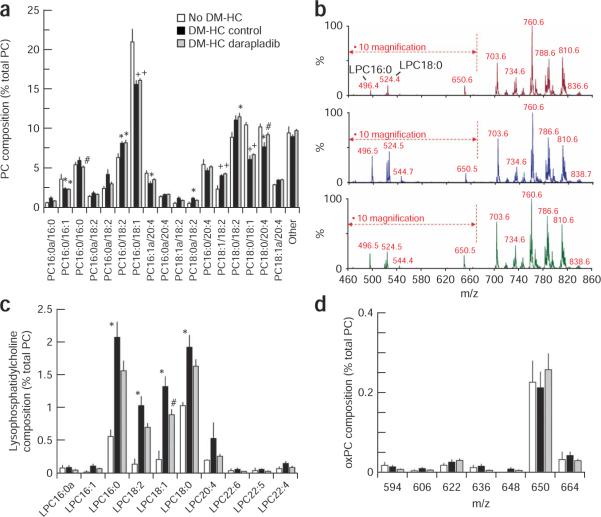
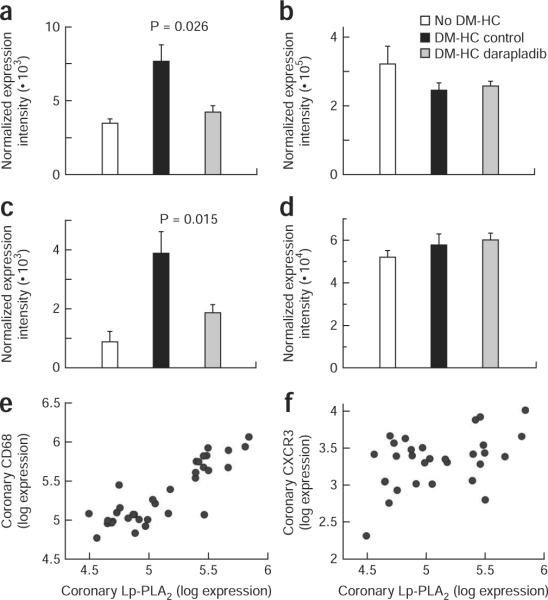
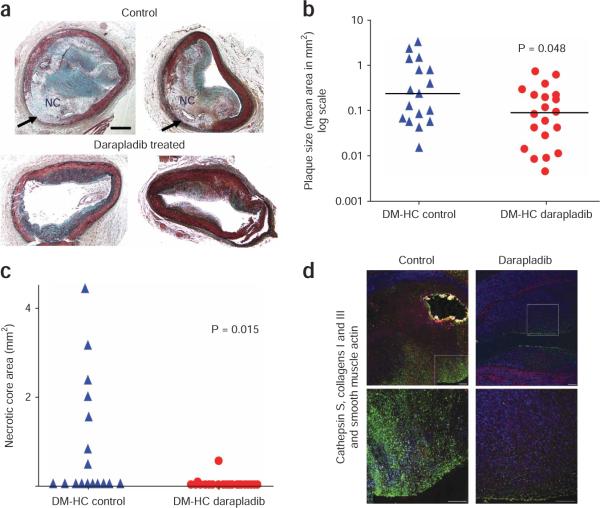
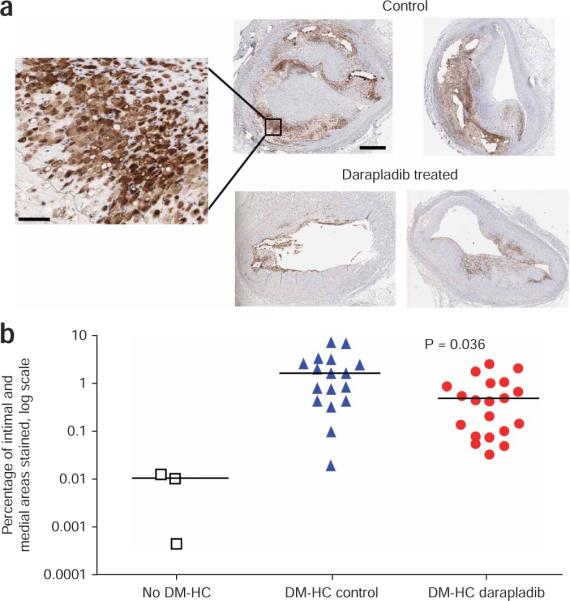
Increased lipoprotein-associated phospholipase A(2) (Lp-PLA(2)) activity is associated with increased risk of cardiac events, but it is not known whether Lp-PLA(2) is a causative agent. Here we show that selective inhibition of Lp-PLA(2) with darapladib reduced development of advanced coronary atherosclerosis in diabetic and hypercholesterolemic swine. Darapladib markedly inhibited plasma and lesion Lp-PLA(2) activity and reduced lesion lysophosphatidylcholine content. Analysis of coronary gene expression showed that darapladib exerted a general anti-inflammatory action, substantially reducing the expression of 24 genes associated with macrophage and T lymphocyte functioning. Darapladib treatment resulted in a considerable decrease in plaque area and, notably, a markedly reduced necrotic core area and reduced medial destruction, resulting in fewer lesions with an unstable phenotype. These data show that selective inhibition of Lp-PLA(2) inhibits progression to advanced coronary atherosclerotic lesions and confirms a crucial role of vascular inflammation independent from hypercholesterolemia in the development of lesions implicated in the pathogenesis of myocardial infarction and stroke.
Figures
Comment in
-
Getting to the core of atherosclerosis.Nat Med. 2008 Oct;14(10):1015-6. doi: 10.1038/nm1008-1015. Nat Med. 2008. PMID: 18841134 No abstract available.
References
-
- Ross R. Atherosclerosis—an inflammatory disease. N. Engl. J. Med. 1999;340:115–126. - PubMed
-
- Hansson GK, Libby P. The immune response in atherosclerosis: a double-edged sword. Nat. Rev. Immunol. 2006;6:508–519. - PubMed
-
- Steinberg D. Thematic review series: the pathogenesis of atherosclerosis. An interpretive history of the cholesterol controversy, part V: the discovery of the statins and the end of the controversy. J. Lipid Res. 2006;47:1339–1351. - PubMed
-
- Witztum JL. The oxidation hypothesis of atherosclerosis. Lancet. 1994;344:793–795. - PubMed
-
- Shah PK. Molecular mechanisms of plaque instability. Curr. Opin. Lipidol. 2007;18:492–499. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
