

Updated guidelines for papanicolaou tests, colposcopy, and human papillomavirus testing in adolescents
- PMID: 18809144
- PMCID: PMC2938015
- DOI: 10.1016/j.jadohealth.2008.04.007
Updated guidelines for papanicolaou tests, colposcopy, and human papillomavirus testing in adolescents
Abstract
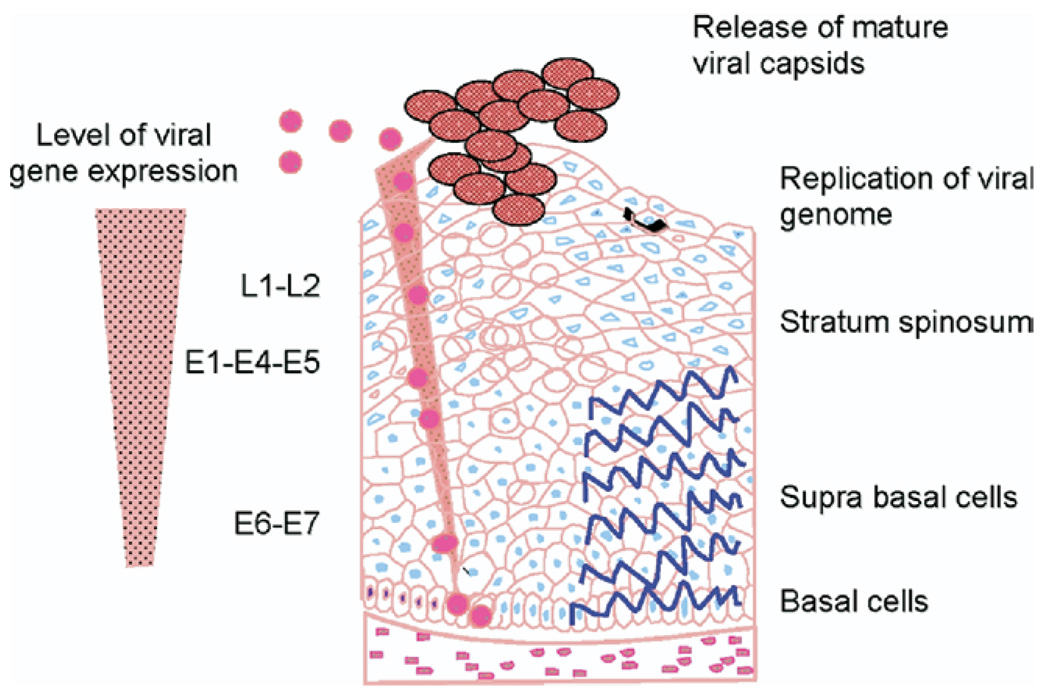
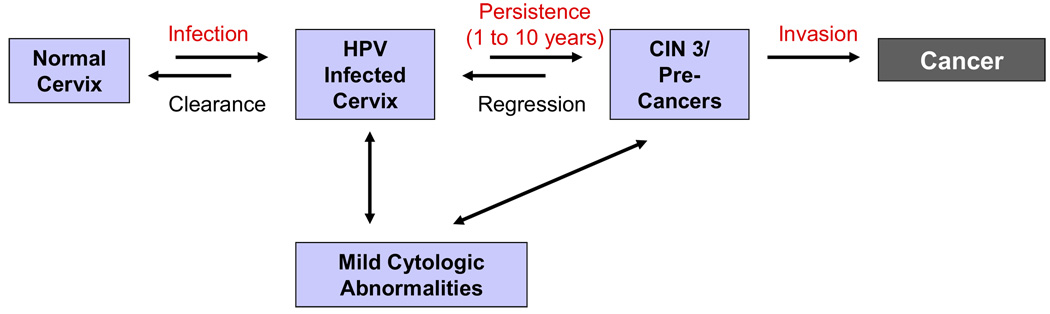
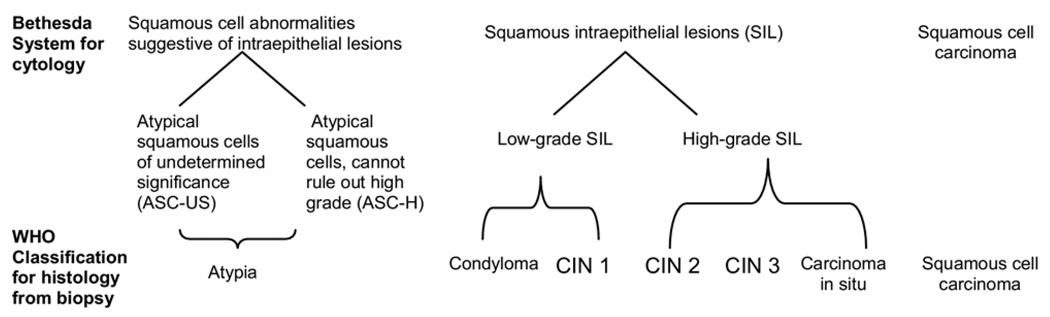
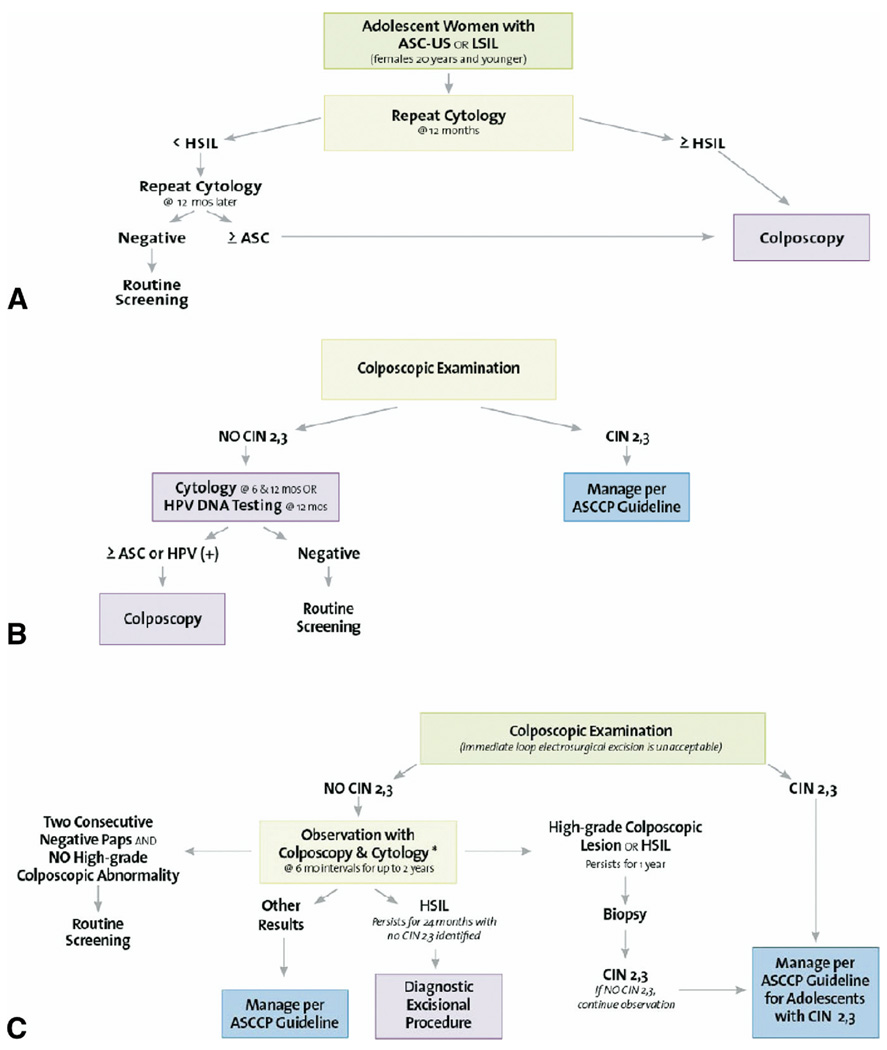
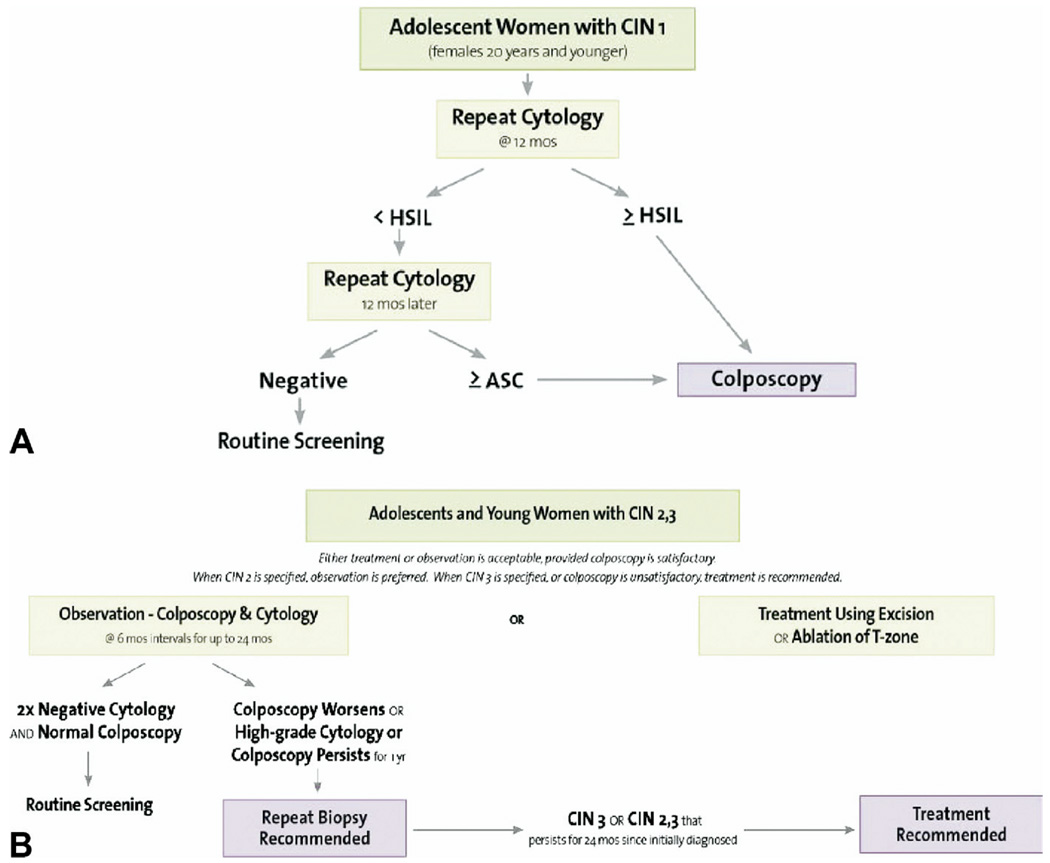
Worldwide, cervical cancer is a major health concern for women of all ages; however the epidemiology and biology of human papillomavirus (HPV) infection differs in female adolescents and adults. In the United States, 50% of adolescent and young women acquire HPV within 3 years after initiating sexual intercourse, resulting in relatively high prevalence rates. Most infections, however, are transient and clear within several months. Consequently HPV infections detected in adolescents are likely to reflect benign disease, whereas infections detected in older women are likely to reflect persistent infections and a higher risk of advanced cervical intraepithelial lesions that can lead to invasive cervical cancer. This article reviews the most recently published guidelines for the prevention of cervical cancer through screening and management of abnormal cervical cytologic and histologic findings, which have been updated to reflect the differences in HPV infections and cervical abnormalities in female adolescents and adults.
Figures
Similar articles
-
HPV DNA testing of self-collected vaginal samples compared with cytologic screening to detect cervical cancer.JAMA. 2000 Jan 5;283(1):81-6. doi: 10.1001/jama.283.1.81. JAMA. 2000. PMID: 10632284
-
Human papillomavirus (HPV) testing in the management of women with abnormal Pap smears. Experience of a colposcopy referral clinic.Eur J Gynaecol Oncol. 2004;25(5):577-84. Eur J Gynaecol Oncol. 2004. PMID: 15493169
-
Human papillomavirus and Papanicolaou tests to screen for cervical cancer.N Engl J Med. 2007 Oct 18;357(16):1589-97. doi: 10.1056/NEJMoa073204. N Engl J Med. 2007. PMID: 17942872 Clinical Trial.
-
Cervical cytology screening in teens.Curr Womens Health Rep. 2003 Dec;3(6):433-7. Curr Womens Health Rep. 2003. PMID: 14613663 Review.
-
Human papillomavirus testing in primary cervical screening and abnormal Papanicolaou management.Obstet Gynecol Surv. 2006 Jun;61(6 Suppl 1):S15-25. doi: 10.1097/01.ogx.0000221011.01750.25. Obstet Gynecol Surv. 2006. PMID: 16729900 Review.
Cited by
-
Influencing Factors of High-Risk Human Papillomavirus Infection and DNA Load According to the Severity of Cervical Lesions in Female Coal Mine Workers of China.J Cancer. 2019 Oct 6;10(23):5764-5769. doi: 10.7150/jca.29034. eCollection 2019. J Cancer. 2019. PMID: 31737113 Free PMC article.
-
Sexually transmitted diseases treatment guidelines, 2015.MMWR Recomm Rep. 2015 Jun 5;64(RR-03):1-137. MMWR Recomm Rep. 2015. PMID: 26042815 Free PMC article.
-
A Viable and Simple Self-Sampling Method for Human Papillomavirus Detection among South African Adolescents.J Immunol Tech Infect Dis. 2013 Sep 18;2(3):10.4172/2329-9541.1000113. doi: 10.4172/2329-9541.1000113. J Immunol Tech Infect Dis. 2013. PMID: 24324979 Free PMC article.
-
HPV infection and cervical neoplasia: associated risk factors.Infect Agent Cancer. 2015 May 26;10:16. doi: 10.1186/s13027-015-0011-3. eCollection 2015. Infect Agent Cancer. 2015. PMID: 26244052 Free PMC article.
-
Cervical cancer knowledge and prevention among college women.J Community Health. 2013 Dec;38(6):997-1002. doi: 10.1007/s10900-013-9707-8. J Community Health. 2013. PMID: 23715964
References
-
- Ferlay J, et al. IARC Cancer Base No. 5 Version 2.0. Lyon, France: IARC Press; 2002. GLOBOCAN 2002: Cancer Incidence, Mortality and Prevalence Worldwide; p. 2004.
-
- Doorbar J. Molecular biology of human papillomavirus infection and cervical cancer. Clin Sci (Lond) 2006;110:525–541. - PubMed
-
- Muñoz N, et al. Epidemiologic classification of human papillomavirus types associated with cervical cancer. N Engl J Med. 2003;348:518–527. - PubMed
-
- Trottier H, Franco EL. The epidemiology of genital human papillomavirus infection. Vaccine. 2006;24 Suppl 1:S1–S15. - PubMed
-
- Woodman CB, et al. Natural history of cervical human papillomavirus infection in young women: A longitudinal cohort study. Lancet. 2001;357:1831–1836. - PubMed
