

Cost-effectiveness of HIV monitoring strategies in resource-limited settings: a southern African analysis
- PMID: 18809819
- PMCID: PMC2894578
- DOI: 10.1001/archinternmed.2008.1
Cost-effectiveness of HIV monitoring strategies in resource-limited settings: a southern African analysis
Abstract
Background: Although the number of infected persons receiving highly active antiretroviral therapy (HAART) in low- and middle-income countries has increased dramatically, optimal disease management is not well defined.
Methods: We developed a model to compare the costs and benefits of 3 types of human immunodeficiency virus monitoring strategies: symptom-based strategies, CD4-based strategies, and CD4 counts plus viral load strategies for starting, switching, and stopping HAART. We used clinical and cost data from southern Africa and performed a cost-effectiveness analysis. All assumptions were tested in sensitivity analyses.
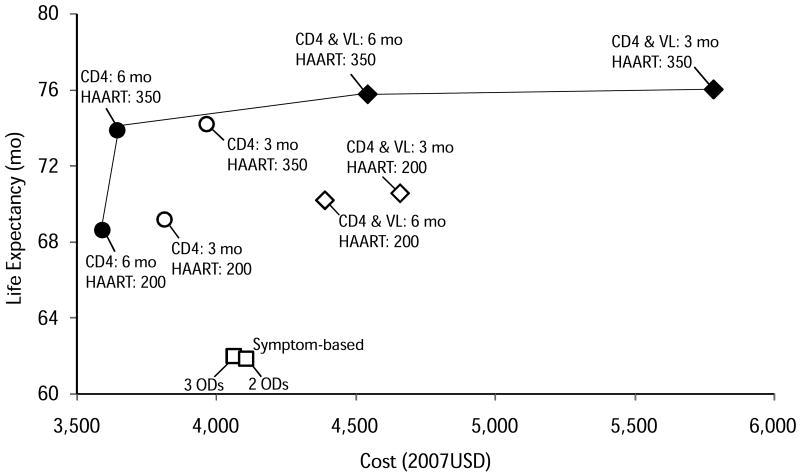
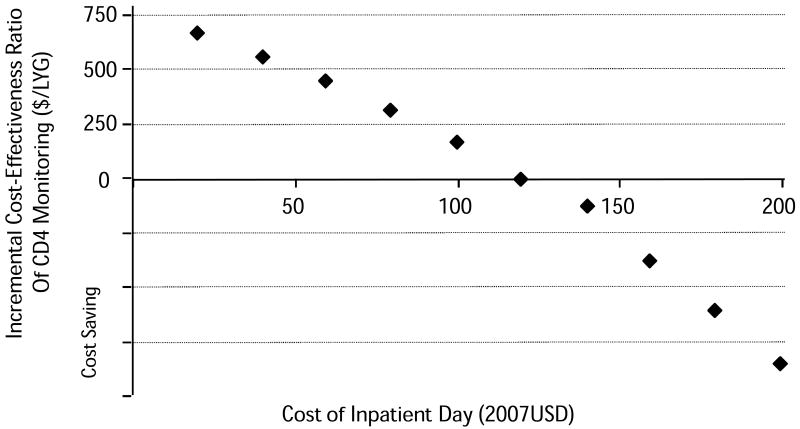
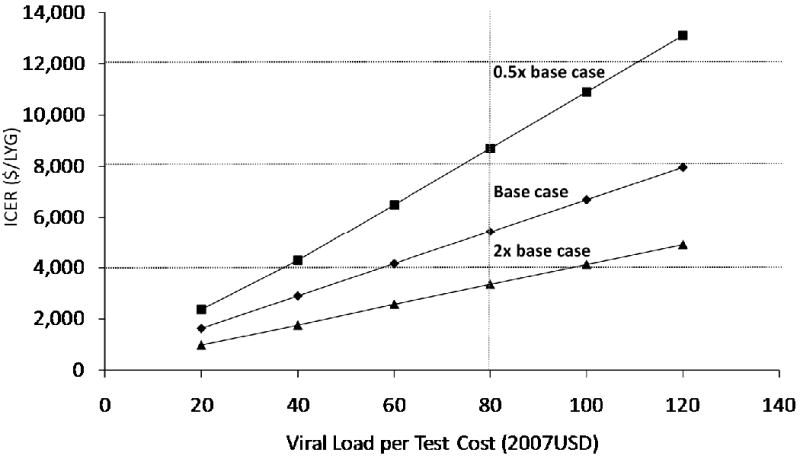
Results: Compared with the symptom-based approaches, monitoring CD4 counts every 6 months and starting treatment at a threshold of 200/muL was associated with a gain in life expectancy of 6.5 months (61.9 months vs 68.4 months) and a discounted lifetime cost savings of US $464 per person (US $4069 vs US $3605, discounted 2007 dollars). The CD4-based strategies in which treatment was started at the higher threshold of 350/microL provided an additional gain in life expectancy of 5.3 months at a cost-effectiveness of US $107 per life-year gained compared with a threshold of 200/microL. Monitoring viral load with CD4 was more expensive than monitoring CD4 counts alone, added 2.0 months of life, and had an incremental cost-effectiveness ratio of US $5414 per life-year gained relative to monitoring of CD4 counts. In sensitivity analyses, the cost savings from CD4 count monitoring compared with the symptom-based approaches was sensitive to cost of inpatient care, and the cost-effectiveness of viral load monitoring was influenced by the per test costs and rates of virologic failure.
Conclusions: Use of CD4 monitoring and early initiation of HAART in southern Africa provides large health benefits relative to symptom-based approaches for HAART management. In southern African countries with relatively high costs of hospitalization, CD4 monitoring would likely reduce total health care expenditures. The cost-effectiveness of viral load monitoring depends on test prices and rates of virologic failure.
Figures
Comment in
-
Cost-effectiveness of strategies for monitoring the response to antiretroviral therapy in resource-limited settings.Arch Intern Med. 2009 May 11;169(9):904; author reply 904-5. doi: 10.1001/archinternmed.2009.88. Arch Intern Med. 2009. PMID: 19433706 No abstract available.
References
-
- UNAIDS. 2006 Report on the Global AIDS Epidemic. Geneva: Joint United Nations Programme on HIV/AIDS; 2006.
-
- UNAIDS. AIDS Epidemic Update. Geneva: 2007.
-
- Hammer S, Havlir D, Klement E, et al. Scaling up Antiretroviral Therapy in Resource-Limited Settings: Treatment Guidelines for a Public health Approach. Geneva: World Health Organization; 2003.
-
- Bishai D, Colchero A, Durack DT. The cost effectiveness of antiretroviral treatment strategies in resource-limited settings. AIDS. 2007;21(10):1333–1340. - PubMed
-
- Stover J, Walker N, Garnett GP, et al. Can we reverse the HIV/AIDS pandemic with an expanded response? The lancet. 2002;360(9326):73–77. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
