

Childhood sarcoidosis: A rare but fascinating disorder
- PMID: 18811966
- PMCID: PMC2559831
- DOI: 10.1186/1546-0096-6-16
Childhood sarcoidosis: A rare but fascinating disorder
Abstract
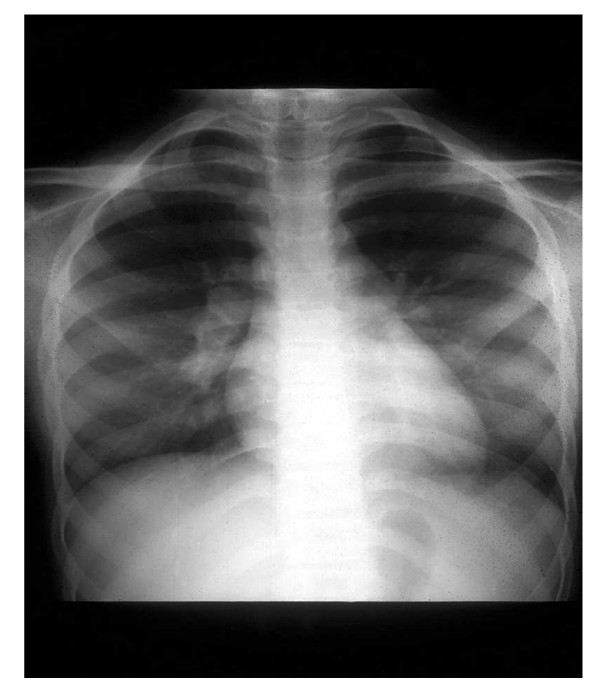
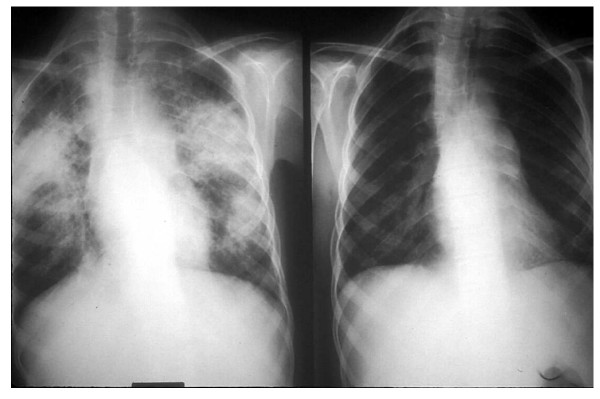
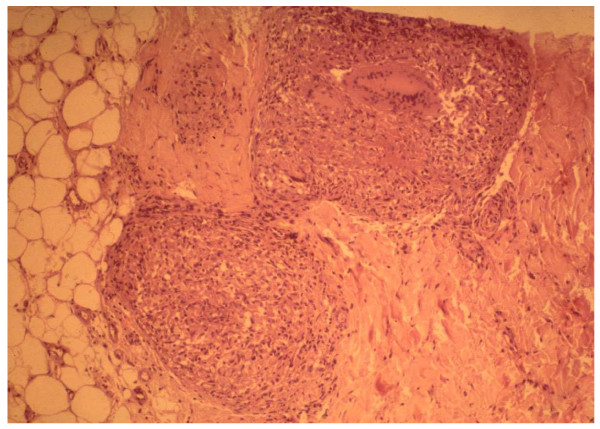
Childhood sarcoidosis is a rare multisystemic granulomatous disorder of unknown etiology. In the pediatric series reported from the southeastern United States, sarcoidosis had a higher incidence among African Americans. Most reported childhood cases have occurred in patients aged 13-15 years. Macrophages bearing an increased expression of major histocompatibility class (MHC) II molecules most likely initiate the inflammatory response of sarcoidosis by presenting an unidentified antigen to CD4+ Th (helper-inducer) lymphocytes. A persistent, poorly degradable antigen driven cell-mediated immune response leads to a cytokine cascade, to granuloma formation, and eventually to fibrosis. Frequently observed immunologic features include depression of cutaneous delayed-type hypersensitivity and a heightened helper T cell type 1 (Th1) immune response at sites of disease. Circulating immune complexes, along with signs of B cell hyperactivity, may also be found. The clinical presentation can vary greatly depending upon the organs involved and age of the patient. Two distinct forms of sarcoidosis exist in children. Older children usually present with a multisystem disease similar to the adult manifestations, with frequent hilar lymphadenopathy and pulmonary infiltrations. Early-onset sarcoidosis is a unique form of the disease characterized by the triad of rash, uveitis, and arthritis in children presenting before four years of age. The diagnosis of sarcoidosis is confirmed by demonstrating a typical noncaseating granuloma on a biopsy specimen. Other granulmatous diseases should be reasonably excluded. The current therapy of choice for sarcoidosis in children with multisystem involvement is oral corticosteroids. Methotrexate given orally in low doses has been effective, safe and steroid sparing in some patients. Alternative immunosuppressive agents, such as azathioprine, cyclophosphamide, chlorambucil, and cyclosporine, have been tried in adult cases of sarcoidosis with questionable efficacy. The high toxicity profile of these agents, including an increased risk of lymphoproliferative disorders and carcinomas, has limited their use to patients with severe disease refractory to other agents. Successful steroid sparing treatment with mycophenolate mofetil was described in an adolescent with renal-limited sarcoidosis complicated by renal failure. Novel treatment strategies for sarcoidosis have been developed including the use of TNF-alpha inhibitors, such as infliximab. The long-term course and prognosis is not well established in childhood sarcoidosis, but it appears to be poorer in early-onset disease.
Figures

References
-
- Hunninghake GW, Costable U, Ando M, Baughman R, Cordier JF, du Bois R, Eklund A, Kitaichi M, Lynch J, Rizzato G, Selroos O, Semenzato G, Sharma OP. ATS/ERS/WASOG statement of sarcoidosis. American Thoracic Society/European Respiratory Society/World Association of Sarcoidosis and other Granulomatous Disorders. Sarcoidosis Vasc Diffuse Lung Dis. 1999;16:149–173. - PubMed
-
- Hetherington S. Sarcoidosis in young children. Am J Dis Child. 1982;136:13–15. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
