

A polymicrobial perspective of pulmonary infections exposes an enigmatic pathogen in cystic fibrosis patients
- PMID: 18812504
- PMCID: PMC2567494
- DOI: 10.1073/pnas.0804326105
A polymicrobial perspective of pulmonary infections exposes an enigmatic pathogen in cystic fibrosis patients
Abstract
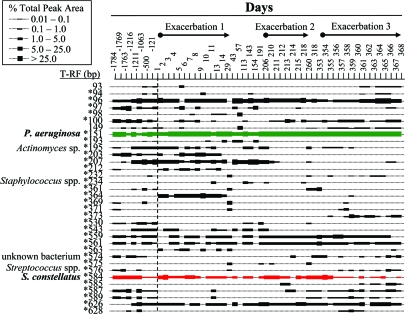
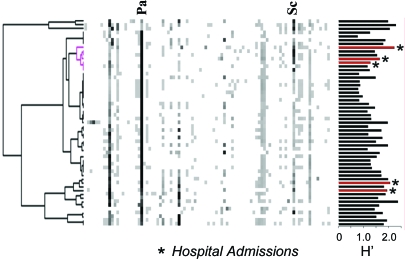
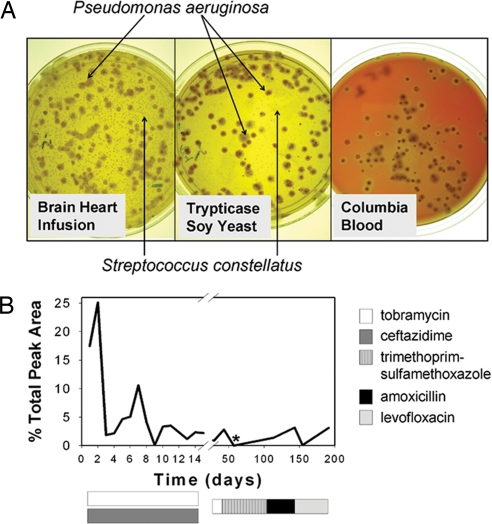
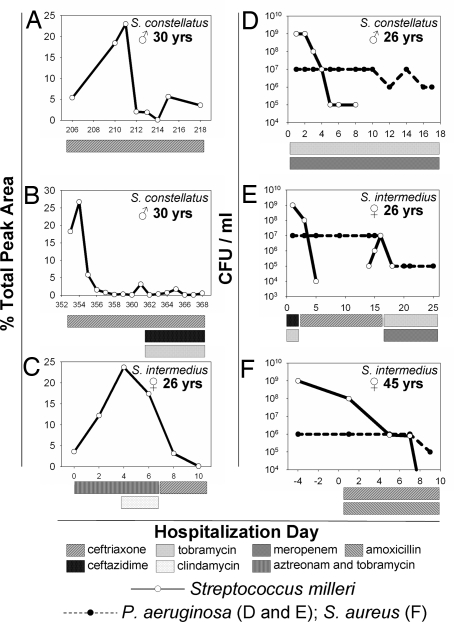
Lung disease is the leading cause of morbidity and mortality in cystic fibrosis (CF) patients. A modest number of bacterial pathogens have been correlated with pulmonary function decline; however, microbiological and molecular evidence suggests that CF airway infection is polymicrobial. To obtain a more complete assessment of the microbial community composition and dynamics, we undertook a longitudinal study by using culture-independent and microbiological approaches. In the process, we demonstrated that within complex and dynamic communities, the Streptococcus milleri group (SMG) can establish chronic pulmonary infections and at the onset of 39% of acute pulmonary exacerbations, SMG is the numerically dominant pathogen. We report the comprehensive polymicrobial community dynamics of a CF lung infection in a clinically relevant context. If a given organism, such as Pseudomonas aeruginosa, becomes resistant to antibiotic therapy, an alternative treatment avenue may mediate the desired clinical response by effectively managing the composition of the microbial community.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Matsui H, et al. Evidence for periciliary liquid layer depletion, not abnormal ion composition, in the pathogenesis of cystic fibrosis airways disease. Cell. 1998;95:1005–1015. - PubMed
-
- Goldman MJ, et al. Human beta-defensin-1 is a salt-sensitive antibiotic in lung that is inactivated in cystic fibrosis. Cell. 1997;88:553–560. - PubMed
-
- Smith JJ, Travis SM, Greenberg EP, Welsh MJ. Cystic fibrosis airway epithelia fail to kill bacteria because of abnormal airway surface fluid. Cell. 1996;85:229–236. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
