

Review
doi: 10.1056/NEJMra0802714.
Lung cancer
Affiliations
- PMID: 18815398
- PMCID: PMC10662965
- DOI: 10.1056/NEJMra0802714
Item in Clipboard
Review
Lung cancer
N Engl J Med.
.
No abstract available
Figures
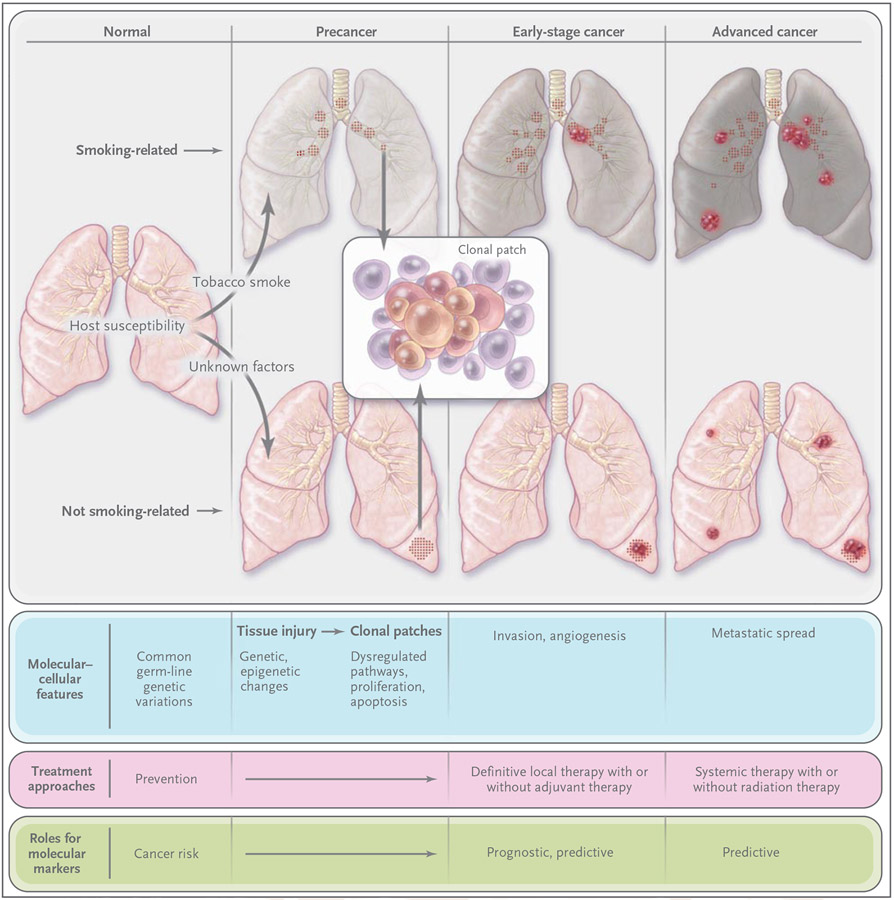
Environmental factors, such as tobacco smoke, and genetic susceptibility interact to influence carcinogenesis. Factors that are unrelated to smoking — including genetic, hormonal, and viral (e.g., human papillomavirus) factors — have been suggested. Tissue injury (e.g., from tobacco smoke, reflected in the discolored smoking-related lungs) initially occurs in the form of genetic and epigenetic changes (e.g., mutations, loss of heterozygosity, and promoter methylation) and global transcriptome changes (e.g., inflammation and apoptosis pathways). These changes can persist long term, and eventually lead to aberrant pathway activation and cellular function (e.g., dysregulated proliferation and apoptosis) to produce premalignant changes, including dysplasia and clonal patches. Additional changes can result in angiogenesis, invasion and early-stage cancer, and advanced cancer and metastasis. Many molecular changes in earliest-stage cancer also occur in advanced disease., Premalignant patches contain clones and subclones (inset), which can involve loss of heterozygosity, microsatellite instability, and mutations (e.g., in p53 and epidermal growth factor receptor [EGFR]). Lung cancers unrelated and related to smoking have strikingly different molecular profiles, including those of mutations in p53, KRAS, EGFR, and HER2. Smoking-related patches and primary cancers (usually squamous-cell carcinoma and small-cell lung cancer) most often develop in the central airway., Most tumors that are not related to smoking are adenocarcinomas and develop in the peripheral airways. Molecular markers can signify risk (in people without cancer), prognosis (outcome independent of treatment), and sensitivity to treatment through predictive markers. Such stage-specific markers can span the course of disease from its early stages through its late stages. They also can help define mechanisms of resistance to therapy.
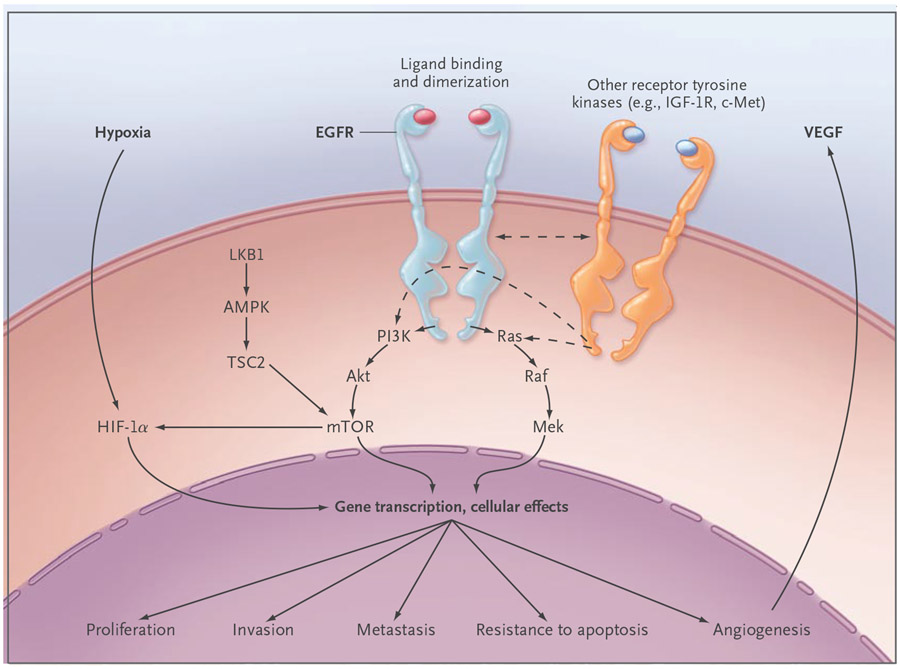
EGFR activates several major downstream signaling pathways, including Ras–Raf–Mek and the pathway consisting of phosphoinositide 3-kinase (PI3K), Akt, and mammalian target of rapamycin (mTOR), which in turn may have an effect on proliferation, survival, invasiveness, metastatic spread, and tumor angiogenesis through pathways that are either dependent on or independent of the hypoxia inducible factor (HIF). These pathways also may be modulated by other receptor tyrosine kinases, such as insulin-like growth factor 1 receptor (IGF-1R) and cMET, and by the LKB1–amp-activated protein kinase (AMPK) pathway, which is involved in energy sensing and cellular stress. Most of these functions depend on signaling through the kinase domain. However, kinase-independent functions, such as maintaining glucose transport, have been reported. TSC2 denotes tuberous sclerosis complex 2, and VEGF vascular endothelial growth factor.
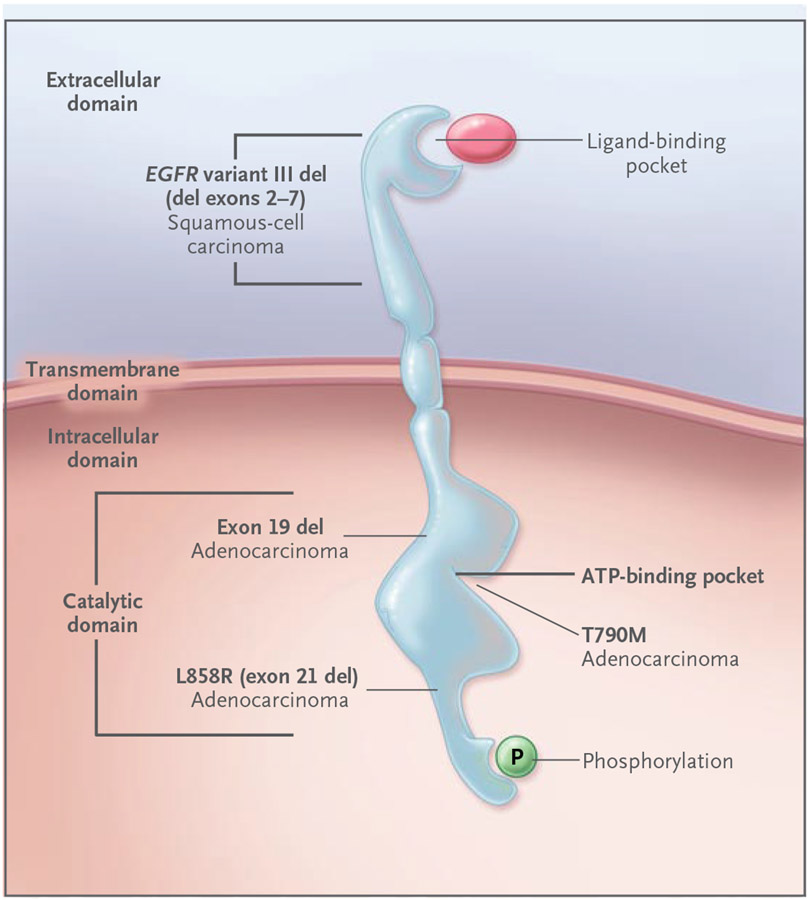
Ligand binding to the EGFR extracellular domain results in receptor homodimerization and tyrosine phosphorylation, with the phosphate derived from ATP bound within the kinase catalytic domain. EGFR mutations have transforming potential in preclinical lung models and can occur early in human lung carcinogenesis. EGFR point mutations (e.g., L858R) and exon 19 deletions, which occur predominantly in adenocarcinoma of the lung, are located within the catalytic domain and result in constitutive EGFR activation. These mutations are associated with increased sensitivity to EGFR tyrosine kinase inhibitors, such as erlotinib and gefitinib. In contrast, mutations in T790M (an amino acid located within the ATP binding site of the EGFR kinase domain) are associated with acquired resistance to these drugs. EGFR variant III mutant deletions occur in the extracellular domain and are associated with squamous-cell cancer.
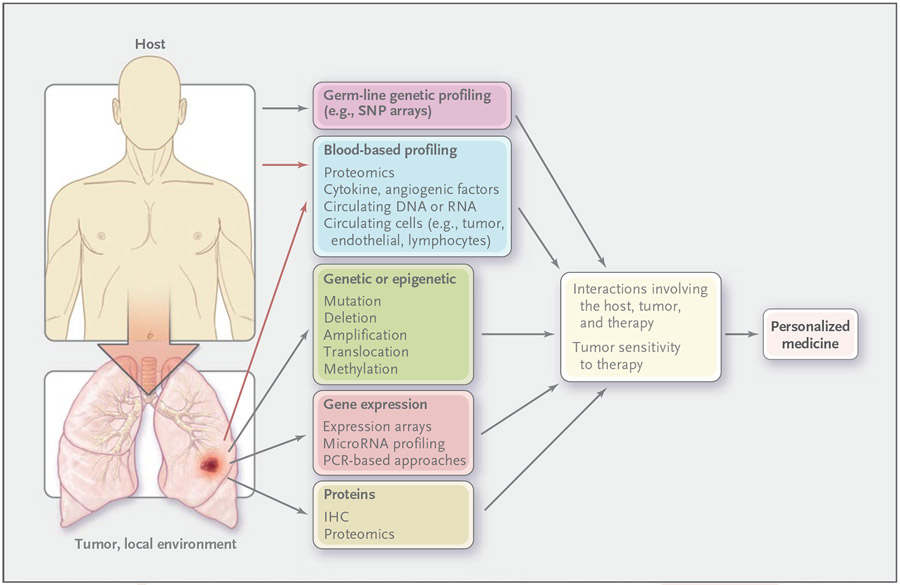
Host profiling involves innate characteristics of the cancer patient. All markers that are involved in profiling lung cancer can apply to the tumor or its local environment. Predictive markers identify groups of patients who are likely to have increased sensitivity or resistance to a given therapy, a critical step in personalizing treatment. It has been traditional to assess individual genetic or protein prognostic or predictive markers (e.g., HER2 for breast cancer), but emerging techniques permit global analyses of the genomic, gene-expression, epigenetic, and protein profiles of the host (innate), including markers in blood and in tumor or nonmalignant lung tissue. These methods include single-nucleotide polymorphism (SNP) arrays to assess genomic alterations, bisulfite sequencing, and methylation-specific polymerase chain reaction (PCR) to assess epigenetic changes, microarrays for assessing gene expression or microRNA levels, and proteomic methods (such as mass spectroscopy, reverse-phase protein arrays, and multiplex beads) to assess intracellular signaling in tumor tissue and cytokines and angiogenic factors in blood. Blood-based profiling includes markers derived from the host (e.g., lymphocytes) and the tumor and local environment (e.g., circulating tumor cells and tumor-derived cytokines) (red arrows). IHC denotes immunohistochemical analysis.
Comment in
-
Lung cancer.N Engl J Med. 2009 Jan 1;360(1):87-8; author reply 88. doi: 10.1056/NEJMc082208. N Engl J Med. 2009. PMID: 19118313 No abstract available.
References
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA Cancer J Clin 2008; 58:71–96. - PubMed
-
- Sun S, Schiller JH, Gazdar AF. Lung cancer in never smokers — a different disease. Nat Rev Cancer 2007;7:778–90. - PubMed
-
- Mao L, Lee JS, Kurie JM, et al. Clonal genetic alterations in the lungs of current and former smokers. J Natl Cancer Inst 1997;89:857–62. - PubMed
-
- Sato M, Shames DS, Gazdar AF, Minna JD. A translational view of the molecular pathogenesis of lung cancer. J Thorac Oncol 2007;2:327–43. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical