

Factors influencing survival after relapse from acute lymphoblastic leukemia: a Children's Oncology Group study
- PMID: 18818707
- PMCID: PMC2872117
- DOI: 10.1038/leu.2008.251
Factors influencing survival after relapse from acute lymphoblastic leukemia: a Children's Oncology Group study
Abstract
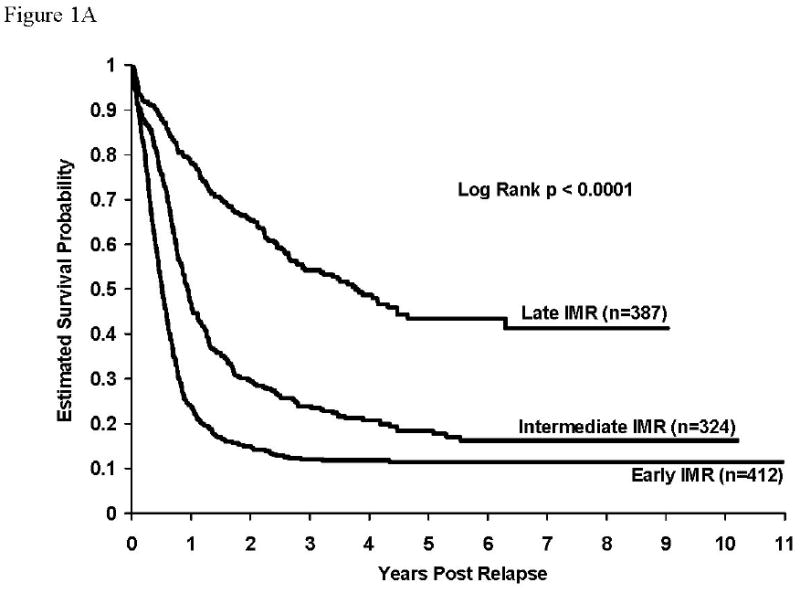
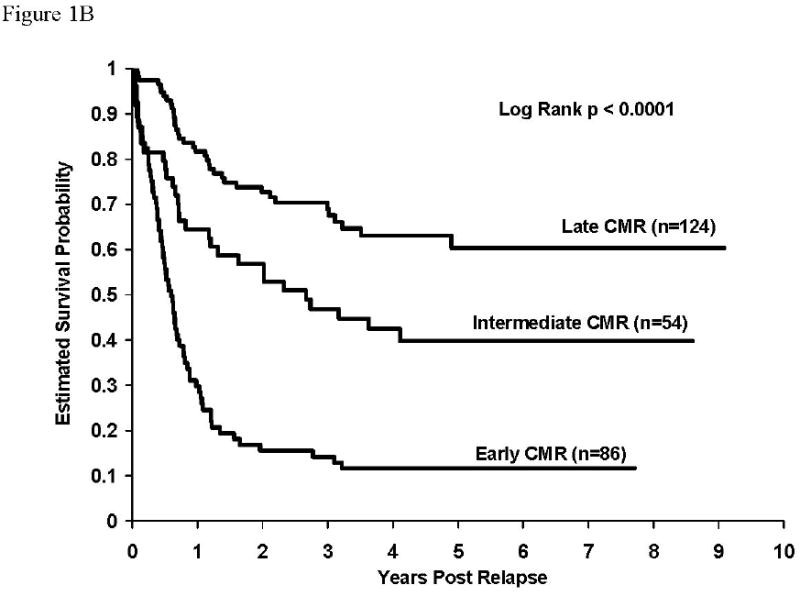
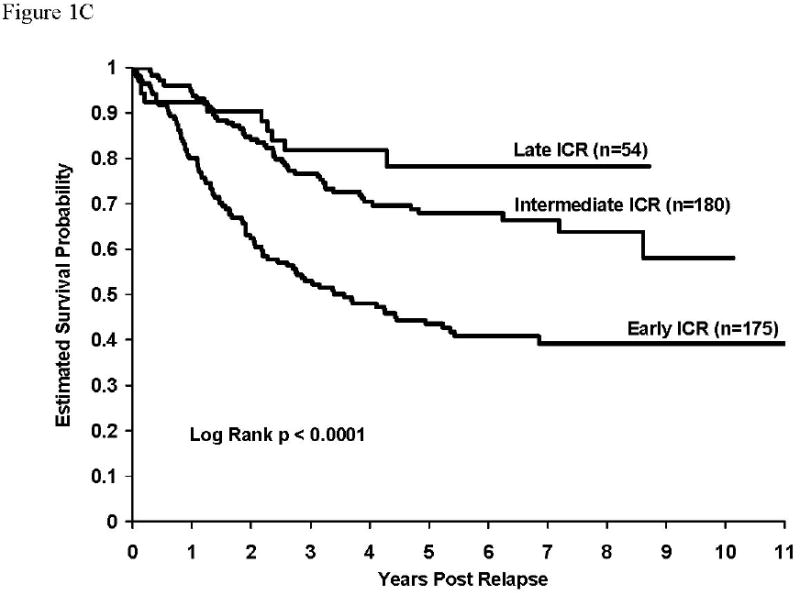
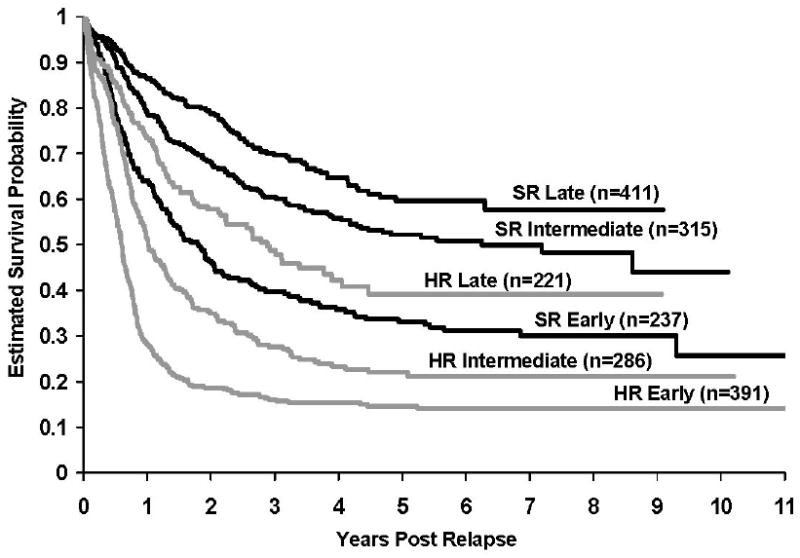
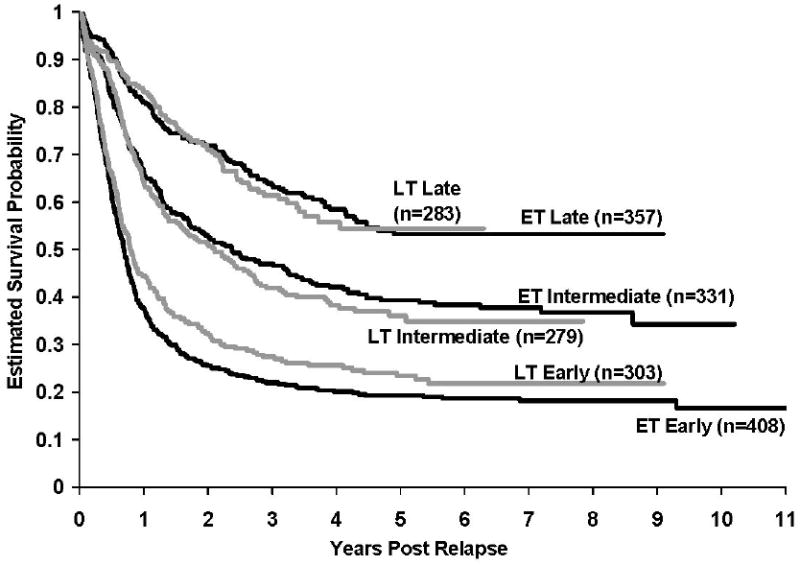
Despite great progress in curing childhood acute lymphoblastic leukemia (ALL), survival after relapse remains poor. We analyzed survival after relapse among 9585 pediatric patients enrolled on Children's Oncology Group clinical trials between 1988 and 2002. A total of 1961 patients (20.5%) experienced relapse at any site. The primary end point was survival. Patients were subcategorized by the site of relapse and timing of relapse from initial diagnosis. Time to relapse remains the strongest predictor of survival. Patients experiencing early relapse less than 18 months from initial diagnosis had a particularly poor outcome with a 5-year survival estimate of 21.0+/-1.8%. Standard risk patients who relapsed had improved survival compared with their higher risk counterparts; differences in survival for the two risk groups was most pronounced for patients relapsing after 18 months. Adjusting for both time and relapse site, multivariate analysis showed that age (10+ years) and the presence of central nervous system disease at diagnosis, male gender, and T-cell disease were significant predictors of inferior post-relapse survival. It can be noted that there was no difference in survival rates for relapsed patients in earlier vs later era trials. New therapeutic strategies are urgently needed for children with relapsed ALL and efforts should focus on discovering the biological pathways that mediate drug resistance.
Figures
References
-
- Pui CH, Evans WE. Treatment of acute lymphoblastic leukemia. N Engl J Med. 2006 Jan 12;354(2):166–78. - PubMed
-
- Jemal A, Siegel R, Ward E, Murray T, Xu J, Smigal C, et al. Cancer statistics, 2006. CA Cancer J Clin. 2006 Mar-Apr;56(2):106–30. - PubMed
-
- Gaynon PS, Trigg ME, Heerema NA, Sensel MG, Sather HN, Hammond GD, et al. Children's Cancer Group trials in childhood acute lymphoblastic leukemia: 1983-1995. Leukemia. 2000 Dec;14(12):2223–33. - PubMed
-
- Henze G, Fengler R, Hartmann R, Kornhuber B, Janka-Schaub G, Niethammer D, et al. Six-year experience with a comprehensive approach to the treatment of recurrent childhood acute lymphoblastic leukemia (ALL-REZ BFM 85). A relapse study of the BFM group. Blood. 1991 Sep 1;78(5):1166–72. - PubMed
-
- Pui CH, Pei D, Sandlund JT, Campana D, Ribeiro RC, Razzouk BI, et al. Risk of adverse events after completion of therapy for childhood acute lymphoblastic leukemia. J Clin Oncol. 2005 Nov 1;23(31):7936–41. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
