

Inherited forms of renal hypomagnesemia: an update
- PMID: 18818955
- PMCID: PMC7811505
- DOI: 10.1007/s00467-008-0968-x
Inherited forms of renal hypomagnesemia: an update
Abstract
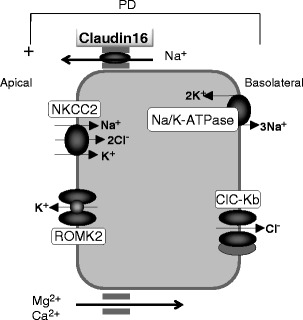
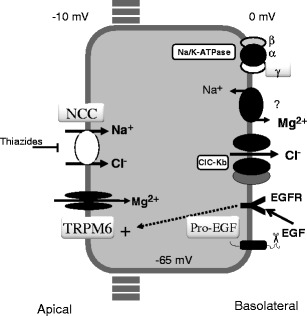
The kidney plays an important role in ion homeostasis in the human body. Several hereditary disorders characterized by perturbations in renal magnesium reabsorption leading to hypomagnesemia have been described over the past 50 years, with the most important of these being Gitelman syndrome, familial hypomagnesemia with hypercalciuria and nephrocalcinosis, familial hypomagnesemia with secondary hypocalcemia, autosomal dominant hypomagnesemia with hypocalciuria, and autosomal recessive hypomagnesemia. Only recently, following positional cloning strategies in affected families, have mutations in renal ion channels and transporters been identified in these diseases. In this short review, I give an update on these hypomagnesemic disorders. Elucidation of the genetic etiology and, for most of these disorders, also the underlying pathophysiology of the disease, has greatly increased our understanding of the normal physiology of renal magnesium handling. This is yet another example of the importance of studying rare disorders in order to unravel physiological and pathophysiological processes in the human body.
Figures
References
-
- Evans RA, Carter JN, George CR, Walls RS, Newland RC, McDonnell GD, Lawrence JR. The congenital “magnesium-loosing kidney”. Report of two patients. QJM. 1981;50:39–52. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Miscellaneous
