

Instability, laxity, and physical function in patients with medial knee osteoarthritis
- PMID: 18820096
- PMCID: PMC2599794
- DOI: 10.2522/ptj.20060223
Instability, laxity, and physical function in patients with medial knee osteoarthritis
Abstract
Background and purpose: Studies have identified factors that contribute to functional limitations in people with knee osteoarthritis (OA), including quadriceps femoris muscle weakness, joint laxity, and reports of knee instability. However, little is known about the relationship among these factors or their relative influence on function. The purpose of this study was to investigate self-reported knee instability and its relationships with knee laxity and function in people with medial knee osteoarthritis (OA).
Participants: Fifty-two individuals with medial knee OA participated in the study.
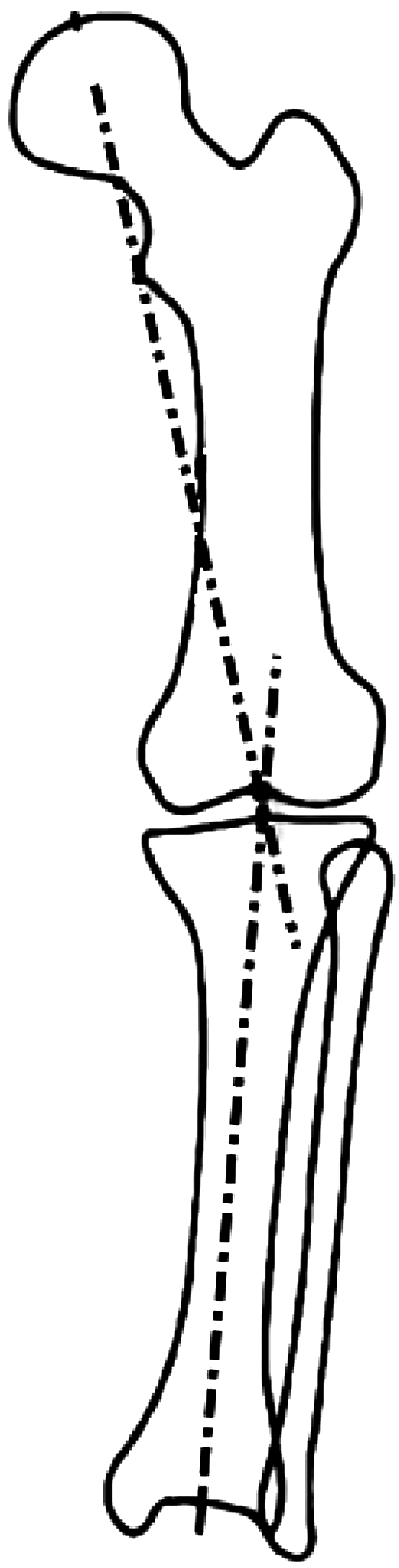
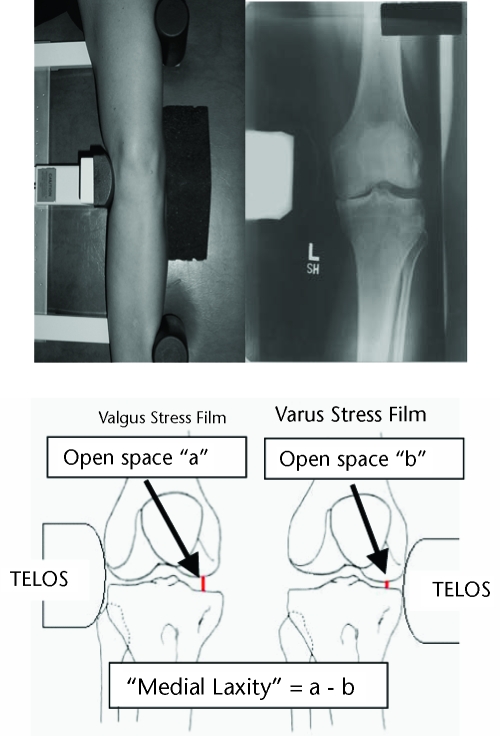
Methods: Each participant was classified into 1 of 3 groups based on reports of knee instability. Limb alignment, knee laxity, and quadriceps femoris muscle strength (force-generating capacity) were assessed. Function was measured with the Knee Injury and Osteoarthritis Outcome Score (KOOS) and a stair-climbing test (SCT). Group differences were detected with one-way analyses of variance, and relationships among variables were assessed with the Eta(2) statistic and hierarchical regression analysis.
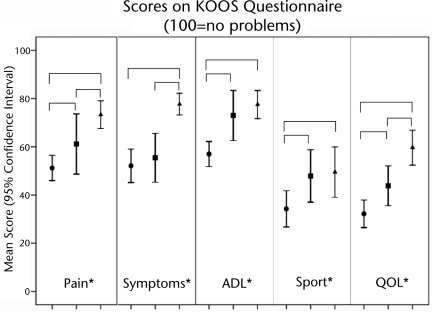
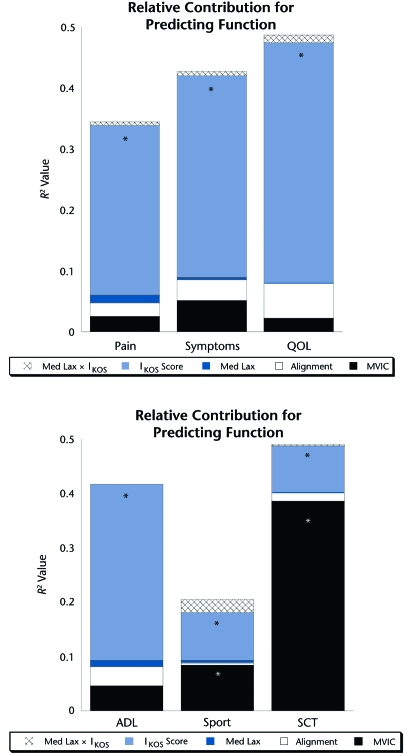
Results: There were no differences in alignment, laxity, or strength among the 3 groups. Self-reported knee instability did not correlate with medial laxity, limb alignment, or quadriceps femoris muscle strength. Individuals reporting worse knee instability scored worse on all subsets of the KOOS. Self-reported knee instability scores significantly contributed to the prediction of all measures of function above that explained by quadriceps femoris muscle force, knee laxity, and alignment. Neither laxity nor alignment contributed to any measure of function.
Discussion and conclusion: Self-reported knee instability is a factor that is not directly associated with knee laxity and contributes to worse function. Further research is necessary to delineate the factors that contribute to self-reported knee instability and reduced function in this population.
Figures
References
-
- Felson DT, Zhang Y, Hannon MT, et al. Risk factors for incident radiographic knee osteoarthritis in the elderly: the Framingham Study. Arthritis Rheum. 1997;40:728–733. - PubMed
-
- McAlindon TE, Wilson PW, Aliabadi P, et al. Level of physical activity and the risk of radiographic and symptomatic knee osteoarthritis in the elderly: the Framingham Study. Am J Med. 1999;106:151–157. - PubMed
-
- Ghosh P, Smith M. Osteoarthritis, genetic and molecular mechanisms. Biogerontology. 2002;3:85–88. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
