

A meta-analysis of the vascular-related safety profile and efficacy of alpha-adrenergic blockers for symptoms related to benign prostatic hyperplasia
- PMID: 18822025
- PMCID: PMC2658011
- DOI: 10.1111/j.1742-1241.2008.01880.x
A meta-analysis of the vascular-related safety profile and efficacy of alpha-adrenergic blockers for symptoms related to benign prostatic hyperplasia
Abstract
Objectives: To evaluate the safety profile and efficacy of alpha1-adrenergic receptor blockers (A1Bs) currently prescribed for benign prostatic hyperplasia (BPH).
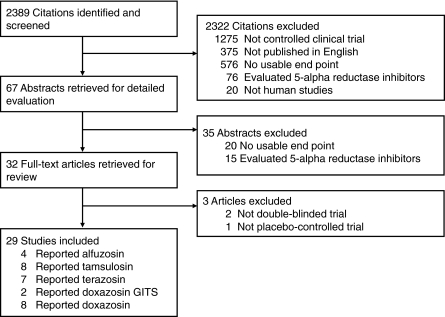
Data sources: A systematic literature search of MEDLINE, the Cochrane Database and the Food and Drug Administration Web site through December 2006 identified double-blinded, prospective, placebo-controlled trials, evaluating agents commercially available by prescription for the symptomatic treatment of BPH.
Review methods: Data were reviewed by two investigators with the use of a standardised data abstraction form. Studies were evaluated for methodological quality using the Jadad scale. Studies with a score of < 3 were considered of weaker methodology.
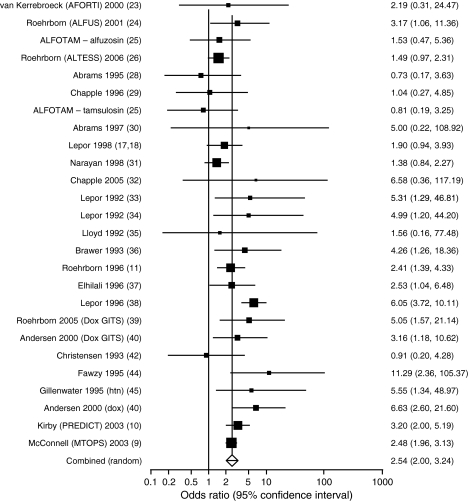
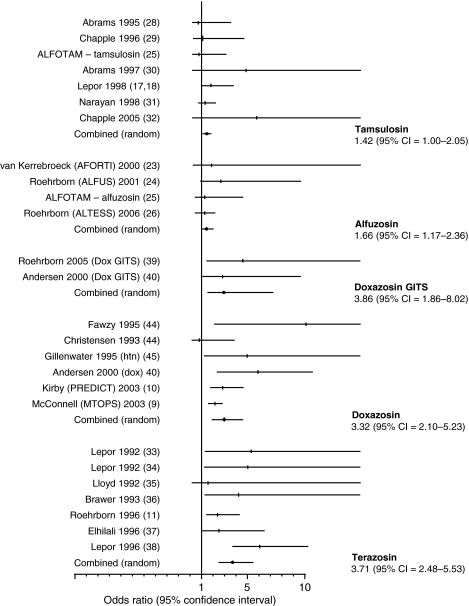
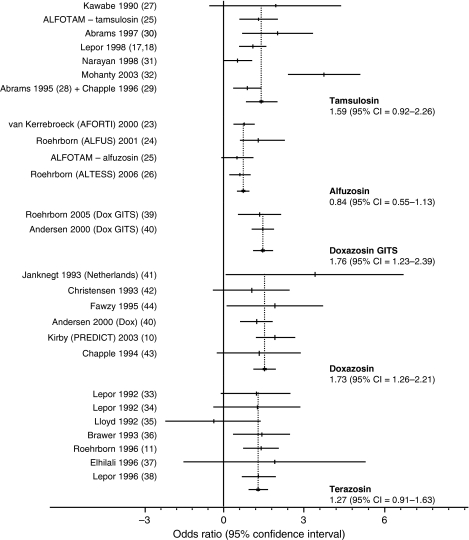
Results: Of 2389 potential citations, 25 were usable for evaluation of safety data, 26 for efficacy. A1B use was associated with a statistically significant increase in the odds of developing a vascular-related event [odds ratio (OR) 2.54; 95% confidence interval (CI): 2.00-3.24; p < 0.0001]. The odds of developing a vascular-related adverse event were: alfuzosin, OR 1.66, 95% CI: 1.17-2.36; terazosin, OR 3.71, 95% CI: 2.48-5.53; doxazosin, OR 3.32, 95% CI: 2.10-5.23 and tamsulosin, OR 1.42, 95% CI: 0.99-2.05. A1Bs increased Q(max) by 1.32 ml/min (95% CI: 1.07-1.57) compared with placebo. Difference from placebo in American Urological Association symptom index/International Prostate Symptom Score was -1.92 points (95% CI: -2.71 to -1.14).
Conclusions: Alfuzosin, terazosin and doxazosin showed a statistically significant increased risk of developing vascular-related events compared with placebo. Tamsulosin showed a numerical increase that was not statistically significant. All agents significantly improved Q(max) and symptom signs compared with placebo.
Figures
References
-
- Boyle P, Napalkov P. The epidemiology of benign prostatic hyperplasia and observations on concomitant hypertension. Scand J Urol Nephrol Suppl. 1995;168:7–12. - PubMed
-
- AUA Practice Guidelines Committee AUA guideline on management of benign prostatic hyperplasia. Chapter 1: Diagnosis and treatment recommendations. J Urol. 2003;170(2 part 1):530–47. - PubMed
-
- Bertaccini A, Vassallo F, Martino F, et al. Symptoms, bothersomeness and quality of life in patients with LUTS suggestive of BPH. Eur Urol. 2001;40(Suppl. 1):13–8. - PubMed
-
- Hargreave TB, McNeill AS. Acute urinary retention in men: the risks and outcomes with medical therapy. Curr Urol Rep. 2005;6:263–70. - PubMed
-
- Caine M. The present role of alpha-adrenergic blockers in the treatment of benign prostatic hypertrophy. J Urol. 1986;136:1–4. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
