

Exploring the cost-effectiveness of Helicobacter pylori screening to prevent gastric cancer in China in anticipation of clinical trial results
- PMID: 18823009
- PMCID: PMC2597699
- DOI: 10.1002/ijc.23864
Exploring the cost-effectiveness of Helicobacter pylori screening to prevent gastric cancer in China in anticipation of clinical trial results
Abstract
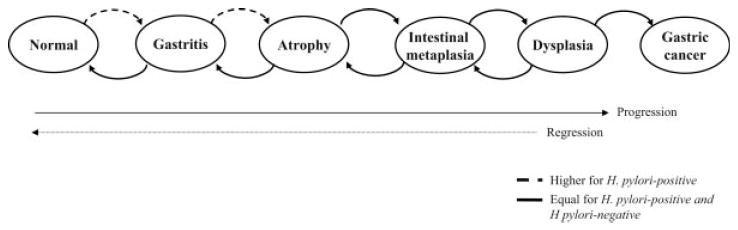
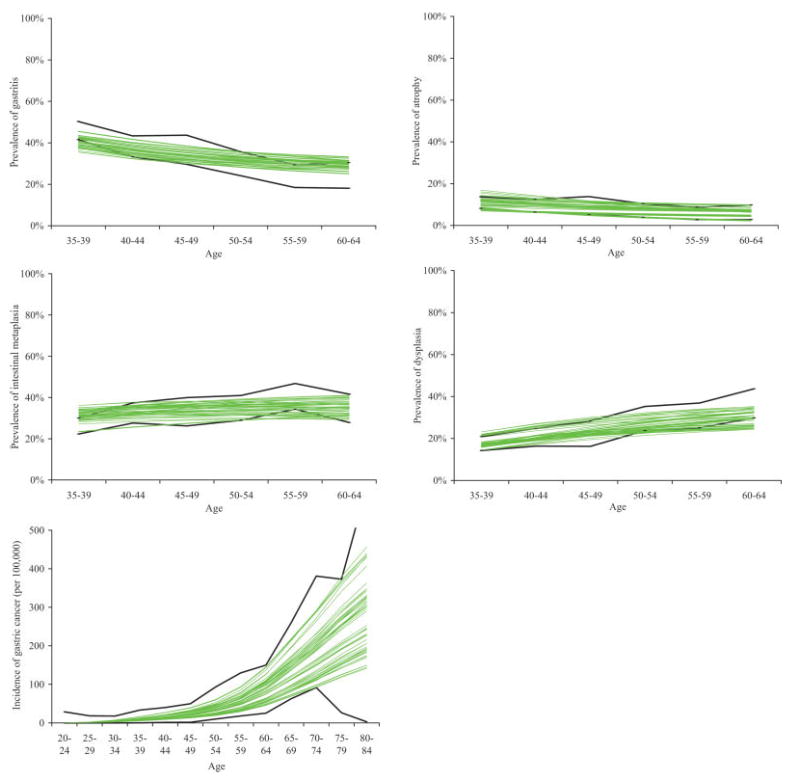
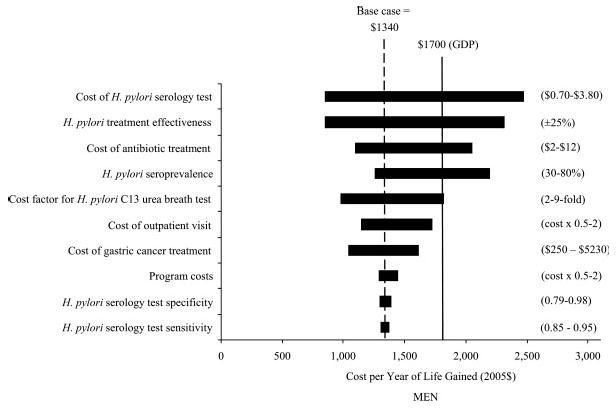
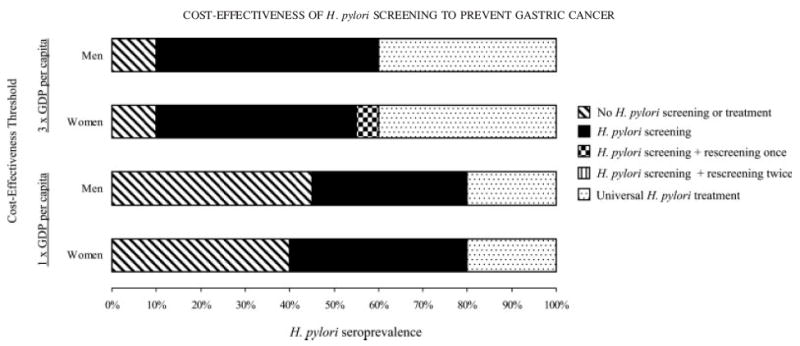
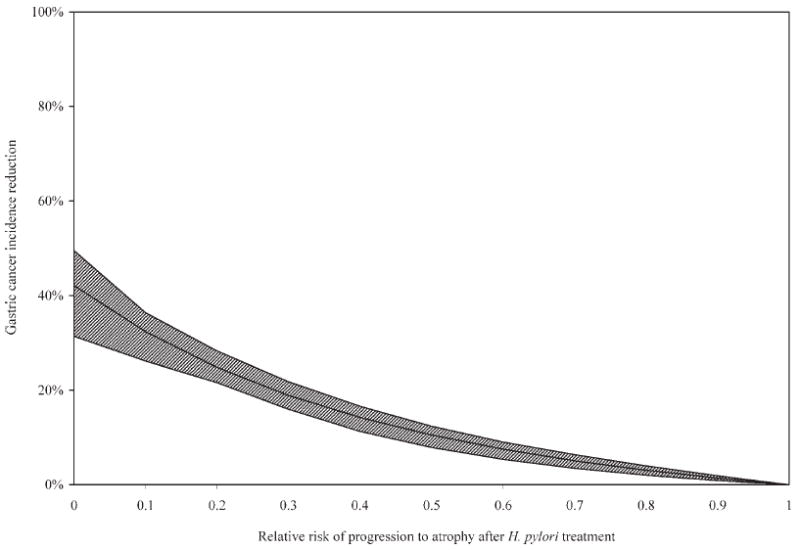
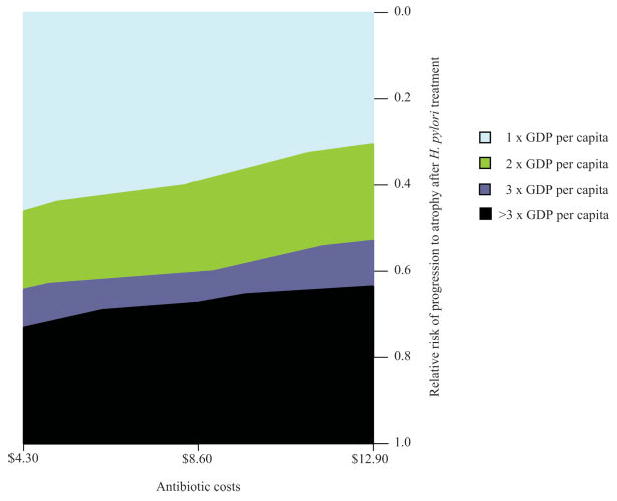
Gastric cancer is the second leading cause of cancer-related deaths worldwide. Treatment for Helicobacter pylori infection, the leading causal risk factor, can reduce disease progression, but the long-term impact on cancer incidence is uncertain. Using the best available data, we estimated the potential health benefits and economic consequences associated with H. pylori screening in a high-risk region of China. An empirically calibrated model of gastric cancer was used to project reduction in lifetime cancer risk, life-expectancy and costs associated with (i) single lifetime screening (age 20, 30 or 40); (ii) single lifetime screening followed by rescreening individuals with negative results and (iii) universal treatment for H. pylori (age 20, 30 or 40). Data were from the published literature and national and international databases. Screening and treatment for H. pylori at age 20 reduced the mean lifetime cancer risk by 14.5% (men) to 26.6% (women) and cost less than $1,500 per year of life saved (YLS) compared to no screening. Rescreening individuals with negative results and targeting older ages was less cost-effective. Universal treatment prevented an additional 1.5% to 2.3% of risk reduction, but incremental cost-effectiveness ratios exceeded $2,500 per YLS. Screening young adults for H. pylori could prevent one in every 4 to 6 cases of gastric cancer in China and would be considered cost-effective using the GDP per capita threshold. These results illustrate the potential promise of a gastric cancer screening program and provide rationale for urgent clinical studies to move the prevention agenda forward.
Figures
Similar articles
-
Cost-effectiveness of Helicobacter pylori screening followed by eradication treatment for employees in Japan.Epidemiol Infect. 2018 Oct;146(14):1834-1840. doi: 10.1017/S095026881800208X. Epub 2018 Jul 30. Epidemiol Infect. 2018. PMID: 30056808 Free PMC article.
-
Clinical and economic effects of population-based Helicobacter pylori screening to prevent gastric cancer.Arch Intern Med. 1999 Jan 25;159(2):142-8. doi: 10.1001/archinte.159.2.142. Arch Intern Med. 1999. PMID: 9927096
-
Economic evaluation of preventing gastric cancer by eliminating Helicobacter pylori infection in China.Scand J Gastroenterol. 2025 Apr;60(4):327-335. doi: 10.1080/00365521.2025.2473020. Epub 2025 Mar 4. Scand J Gastroenterol. 2025. PMID: 40035736
-
AGA Clinical Practice Update on Screening and Surveillance in Individuals at Increased Risk for Gastric Cancer in the United States: Expert Review.Gastroenterology. 2025 Feb;168(2):405-416.e1. doi: 10.1053/j.gastro.2024.11.001. Epub 2024 Dec 23. Gastroenterology. 2025. PMID: 39718517 Review.
-
Cost-effectiveness of screening and treating Helicobacter pylori for gastric cancer prevention.Best Pract Res Clin Gastroenterol. 2013 Dec;27(6):933-47. doi: 10.1016/j.bpg.2013.09.005. Epub 2013 Sep 27. Best Pract Res Clin Gastroenterol. 2013. PMID: 24182612 Free PMC article. Review.
Cited by
-
Health economic evaluation on population-based Helicobacter pylori eradication and endoscopic screening for gastric cancer prevention.Chin J Cancer Res. 2023 Dec 30;35(6):595-605. doi: 10.21147/j.issn.1000-9604.2023.06.04. Chin J Cancer Res. 2023. PMID: 38204445 Free PMC article.
-
Cost-utility analysis of the newly recommended adjuvant chemotherapy for resectable gastric cancer patients in the 2011 Chinese National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology: Gastric Cancer.Pharmacoeconomics. 2014 Mar;32(3):235-43. doi: 10.1007/s40273-013-0065-2. Pharmacoeconomics. 2014. PMID: 23709451
-
Diagnosis and Management of Gastric Intestinal Metaplasia: Current Status and Future Directions.Gut Liver. 2019 Nov 15;13(6):596-603. doi: 10.5009/gnl19181. Gut Liver. 2019. PMID: 31394893 Free PMC article. Review.
-
Gastric biopsies: the gap between evidence-based medicine and daily practice in the management of gastric Helicobacter pylori infection.Can J Gastroenterol. 2013 Oct;27(10):e25-30. doi: 10.1155/2013/897423. Can J Gastroenterol. 2013. PMID: 24106732 Free PMC article.
-
Population screening and treatment of Helicobacter pylori infection.Nat Rev Gastroenterol Hepatol. 2017 Apr;14(4):230-240. doi: 10.1038/nrgastro.2016.195. Epub 2017 Jan 5. Nat Rev Gastroenterol Hepatol. 2017. PMID: 28053340 Review.
References
-
- Parkin DM, Pisani P, Ferlay J. Global cancer statistics. CA Cancer J Clin. 1999;49:33–64. - PubMed
-
- Ekstrom AM, Held M, Hansson LE, Engstrand L, Nyren O. Helicobacter pylori in gastric cancer established by CagA immunoblot as a marker of past infection. Gastroenterology. 2001;121:784–91. - PubMed
-
- Ferlay J, Bray F, Pisani P, Parkin DM. IARC cancer base no. 5 version 2.0. Lyon: IARC Press; 2004. GLOBOCAN 2002. Cancer incidence, mortality and prevalence worldwide.
-
- de Vries AC, Haringsma J, Kuipers EJ. The detection, surveillance and treatment of premalignant gastric lesions related to Helicobacter pylori infection. Helicobacter. 2007;12:1–15. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
