

Warfarin use leads to larger intracerebral hematomas
- PMID: 18824672
- PMCID: PMC2668872
- DOI: 10.1212/01.wnl.0000326895.58992.27
Warfarin use leads to larger intracerebral hematomas
Abstract
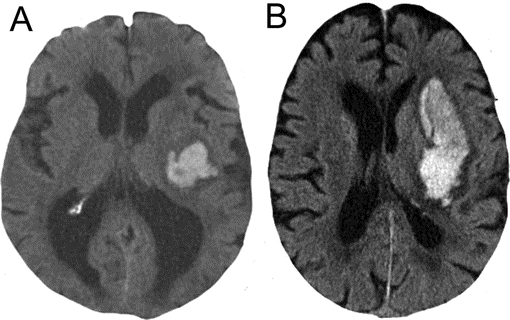
Background: Among patients with intracerebral hemorrhage (ICH), warfarin use before onset leads to greater mortality. In a retrospective study, we sought to determine whether warfarin use is associated with larger initial hematoma volume, one determinant of mortality after ICH.
Methods: We identified all patients hospitalized with ICH in the Greater Cincinnati region from January through December 2005. ICH volumes were measured on the first available brain scan by using the abc/2 method. Univariable analyses and a multivariable generalized linear model were used to determine whether international normalized ratio (INR) influenced initial ICH volume after adjusting for other factors, including age, race, sex, antiplatelet use, hemorrhage location, and time from stroke onset to scan.
Results: There were 258 patients with ICH, including 51 patients taking warfarin. In univariable comparison, when INR was stratified, there was a trend toward a difference in hematoma volume by INR category (INR <1.2, 13.4 mL; INR 1.2-2.0, 9.3 mL; INR 2.1-3.0, 14.0 mL; INR >3.0, 33.2 mL; p = 0.10). In the model, compared with patients with INR <1.2, there was no difference in hematoma size for patients with INR 1.2-2.0 (p = 0.25) or INR 2.1-3.0 (p = 0.36), but patients with INR >3.0 had greater hematoma volume (p = 0.02). Other predictors of larger hematoma size were ICH location (lobar compared with deep cerebral, p = 0.02) and shorter time from stroke onset to scan (p < 0.001).
Conclusion: Warfarin use was associated with larger initial intracerebral hemorrhage (ICH) volume, but this effect was only observed for INR values >3.0. Larger ICH volume among warfarin users likely accounts for part of the excess mortality in this group.
Figures
Similar articles
-
Warfarin-associated intracerebral hemorrhage: volume, anticoagulation intensity and location.J Neurol Sci. 2013 Sep 15;332(1-2):75-9. doi: 10.1016/j.jns.2013.06.020. Epub 2013 Jul 30. J Neurol Sci. 2013. PMID: 23911098
-
Warfarin associated intracerebral hemorrhage in Hong Kong Chinese.Neurol Res. 2014 Feb;36(2):143-9. doi: 10.1179/1743132813Y.0000000275. Epub 2013 Dec 6. Neurol Res. 2014. PMID: 24172661
-
Antithrombotic medications and the etiology of intracerebral hemorrhage: MUCH-Italy.Neurology. 2014 Feb 11;82(6):529-35. doi: 10.1212/WNL.0000000000000108. Epub 2014 Jan 15. Neurology. 2014. PMID: 24431299
-
Predisposing factors for enlargement of intracerebral hemorrhage in patients treated with warfarin.Thromb Haemost. 2003 Feb;89(2):278-83. Thromb Haemost. 2003. PMID: 12574807 Review.
-
Outcome of intracerebral haemorrhage related to non-vitamin K antagonists oral anticoagulants versus vitamin K antagonists: a comprehensive systematic review and meta-analysis.J Neurol Neurosurg Psychiatry. 2018 Mar;89(3):263-270. doi: 10.1136/jnnp-2017-316631. Epub 2017 Oct 13. J Neurol Neurosurg Psychiatry. 2018. PMID: 29030422
Cited by
-
Time to Anticoagulation Reversal and Outcomes After Intracerebral Hemorrhage.JAMA Neurol. 2024 Feb 9;81(4):363-72. doi: 10.1001/jamaneurol.2024.0221. Online ahead of print. JAMA Neurol. 2024. PMID: 38335064 Free PMC article.
-
Computed tomography in acute intracerebral hemorrhage: neuroimaging predictors of hematoma expansion and outcome.Insights Imaging. 2022 Nov 22;13(1):180. doi: 10.1186/s13244-022-01309-1. Insights Imaging. 2022. PMID: 36417131 Free PMC article. Review.
-
Predicting Prognosis of Intracerebral Hemorrhage (ICH): Performance of ICH Score Is Not Improved by Adding Oral Anticoagulant Use.Front Neurol. 2018 Feb 28;9:100. doi: 10.3389/fneur.2018.00100. eCollection 2018. Front Neurol. 2018. PMID: 29541054 Free PMC article.
-
Prestroke physical activity is associated with admission haematoma volume and the clinical outcome of intracerebral haemorrhage.Stroke Vasc Neurol. 2023 Dec 29;8(6):511-520. doi: 10.1136/svn-2023-002316. Stroke Vasc Neurol. 2023. PMID: 37137521 Free PMC article.
-
Intracerebral haemorrhage associated with antithrombotic treatment: translational insights from experimental studies.Lancet Neurol. 2013 Apr;12(4):394-405. doi: 10.1016/S1474-4422(13)70049-8. Epub 2013 Mar 18. Lancet Neurol. 2013. PMID: 23518332 Free PMC article. Review.
References
-
- Flaherty ML, Haverbusch M, Sekar P, et al. Long-term mortality after intracerebral hemorrhage. Neurology 2006;66:1182–1186. - PubMed
-
- Rosand J, Eckman MH, Knudsen KA, Singer DE, Greenberg SM. The effect of warfarin and intensity of anticoagulation on outcome of intracerebral hemorrhage. Arch Intern Med 2004;164:880–884. - PubMed
-
- Flaherty ML, Kissela B, Woo D, et al. The increasing incidence of anticoagulant-associated intracerebral hemorrhage. Neurology 2007;68:116–121. - PubMed
-
- Franke CL, de Jonge J, van Swieten JC, Op de Coul AA, van Gijn J. Intracerebral hematomas during anticoagulant treatment. Stroke 1990;21:726–730. - PubMed
-
- Berwaerts J, Dijkhuizen RS, Robb OJ, Webster J. Prediction of functional outcome and in-hospital mortality after admission with oral anticoagulant-related intracerebral hemorrhage. Stroke 2000;31:2558–2562. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical