

Improving generalist end of life care: national consultation with practitioners, commissioners, academics, and service user groups
- PMID: 18829640
- PMCID: PMC2659492
- DOI: 10.1136/bmj.a1720
Improving generalist end of life care: national consultation with practitioners, commissioners, academics, and service user groups
Abstract
Objective: To identify major concerns of national and local importance in the provision, commissioning, research, and use of generalist end of life care.
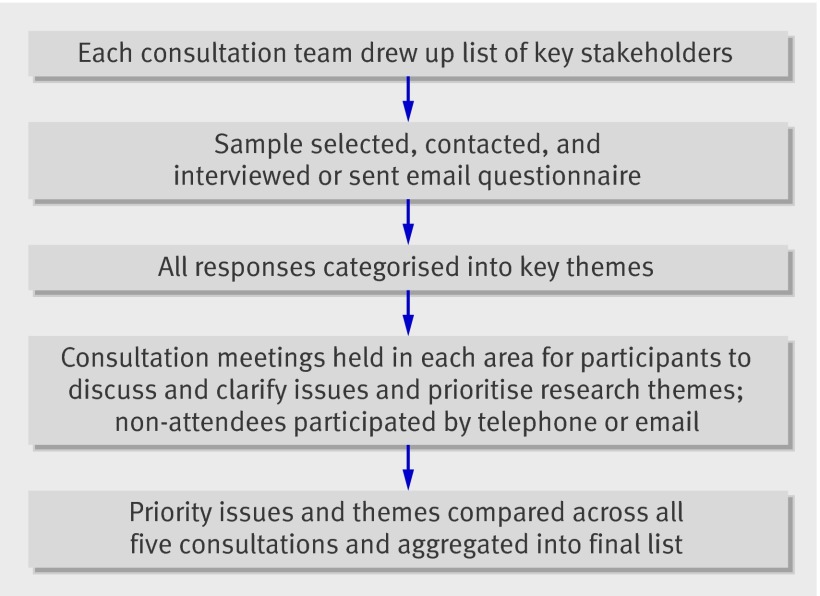
Design: A national consultation and prioritising exercise using a modified form of the nominal group technique.
Participants: Healthcare practitioners, commissioners, academics, and representatives of user and voluntary groups.
Setting: Primary and secondary care, specialist palliative care, and academic and voluntary sectors in England and Scotland.
Results: 74% of those invited (210/285) participated. The stage of life to which "end of life care" referred was not understood in a uniform way. Perceptions ranged from a period of more than a year to the last few days of life. Prominent concerns included difficulties in prognosis and the availability of adequate support for patients with advanced non-malignant disease. Generalists in both primary and secondary care were usually caring for only a few patients approaching the end of life at any one time at a point in time. It was therefore challenging to maintain skills and expertise particularly as educational opportunities were often limited. End of life care took place among many other competing and incentivised activities for general practitioners in the community. More needs to be known about models of end of life care and how these can be integrated in a generalist's workload. A greater evidence base is needed about the effectiveness and application of current tools such as the gold standards framework and Liverpool care pathway and about models of palliation in patients with diseases other than cancer.
Conclusions: Definitions of end of life care need clarification and standardisation. A greater evidence base is needed to define models of good practice together with a commitment to provide education and training and adequate resources for service provision. More needs to be known about the context of provision and the influence of competing priorities and incentives.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Case conferencing - an answer to improving generalist end of life care? Experience from Royal Marsden Hospital.BMJ. 2008 Oct 28;337:a2290. doi: 10.1136/bmj.a2290. BMJ. 2008. PMID: 18957464 No abstract available.
References
-
- Cartwright A. Changes in life and care in the year before death 1969-1987. J Public Health Med 1991;2:81-7. - PubMed
-
- Davies E, Higginson IJ. Palliative care: the solid facts. Denmark: World Health Organization, 2004.
-
- Shugarman LR, Lorenz K, Lynn J. End-of-life care: an agenda for policy improvement. Clin Geriatr Med 2005;21:255-72. - PubMed
-
- Barclay S. Palliative care for non-cancer patients: a UK perspective from primary care. In: Addington-Hall JM, Higginson IJ, eds. Palliative care for non-cancer patients. Oxford: Oxford University Press, 2001.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical