

Development of methodology for conducting clinical trials in frontotemporal lobar degeneration
- PMID: 18829698
- PMCID: PMC2725027
- DOI: 10.1093/brain/awn234
Development of methodology for conducting clinical trials in frontotemporal lobar degeneration
Abstract
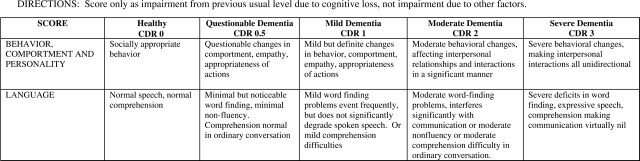
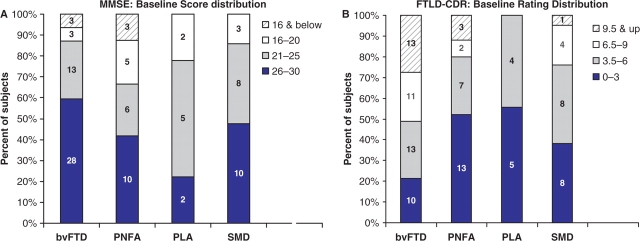
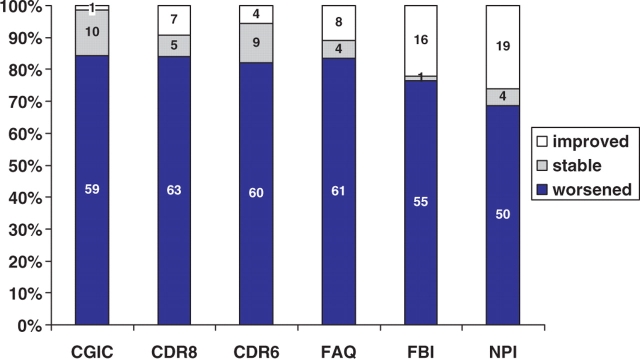
To design clinical trials for the frontotemporal lobar degenerations (FTLD), knowledge about measurement of disease progression is needed to estimate power and enable the choice of optimal outcome measures. The aim here was to conduct a multicentre, 1 year replica of a clinical trial in patients with one of four FTLD syndromes, behavioural variant frontotemporal dementia (bvFTD), progressive nonfluent aphasia (PNFA), progressive logopenic aphasia (PLA) and semantic dementia (SMD). Patients with one of the four FTLD syndromes were recruited from five academic medical centres over a 2 year period. Standard operationalized diagnostic criteria were used. In addition to clinical inclusion and exclusion criteria, patients were required to exhibit focal frontal, temporal or insular brain atrophy or dysfunction by neuroimaging. Patients underwent neuropsychological, functional, behavioural, neurological and MR imaging assessment at baseline and approximately 12 months later. Potential outcome measures were examined for their rates of floor and ceiling values at baseline and end of study, their mean changes and variances. The neuropsychological tests were combined into two cognitive composites -- one for language functions and the other for executive functions. There were 107 patients who underwent baseline assessment and 78 who completed a follow-up assessment within 10-16 months. Two global measures, the FTLD-modified Clinical Dementia Rating (FTLD-modified CDR) and the Clinical Global Impression of Change (CGIC) demonstrated decline in the majority of patients. Several cognitive measures showed negligible floor or ceiling scores either at baseline or follow-up. Scores declined at follow-up in the majority of patients. The cognitive, executive and combined composites were shown to be sensitive to change across all FTLD syndromes. Patients improved at follow-up on the behavioural scales -- the Frontal Behavioural Inventory (22%) and the Neuropsychiatric Inventory (28%) -- suggesting that these instruments may not be ideal for clinical trial use. It was feasible to recruit FTLD patients in a simulated multi-centre trial. There are several candidate outcome measures -- including the FTLD-CDR and the cognitive composites -- that could be used in clinical trials across the spectrum of FTLD.
Figures
References
-
- Aisen PS, Schafer KA, Grundman M, Pfeiffer E, Sano M, Davis KL, et al. Effects of rofecoxib or naproxen vs placebo on Alzheimer disease progression: a randomized controlled trial. JAMA. 2003;289:2819–26. - PubMed
-
- Boxer AL, Boeve BF. Frontotemporal Dementia Treatment: Current Symptomatic Therapies and Implications of Recent Genetic, Biochemical, and Neuroimaging Studies. Alzheimer Dis Assoc Disord. 2007;21:S79–87. - PubMed
-
- Cummings JL, Mega M, Gray K, Rosenberg-Thompson S, Carusi DA, Gornbein J. The Neuropsychiatric Inventory: comprehensive assessment of psychopathology in dementia. Neurology. 1994;44:2308–14. - PubMed
-
- Deakin JB, Rahman S, Nestor PJ, Hodges JR, Sahakian BJ. Paroxetine does not improve symptoms and impairs cognition in frontotemporal dementia: a double-blind randomized controlled trial. Psychopharmacology (Berl) 2004;172:400–8. - PubMed
-
- Delis DC, Kramer JH, Kaplan E, Ober BA. California Verbal Learning Test. 2nd. San Antonio, TX: The Psychological Crop;; 2000.
