

Optimal imaging strategies to assess coronary blood flow and risk for patients with coronary artery disease
- PMID: 18830076
- PMCID: PMC3954509
- DOI: 10.1097/HCO.0b013e328312c2f5
Optimal imaging strategies to assess coronary blood flow and risk for patients with coronary artery disease
Abstract
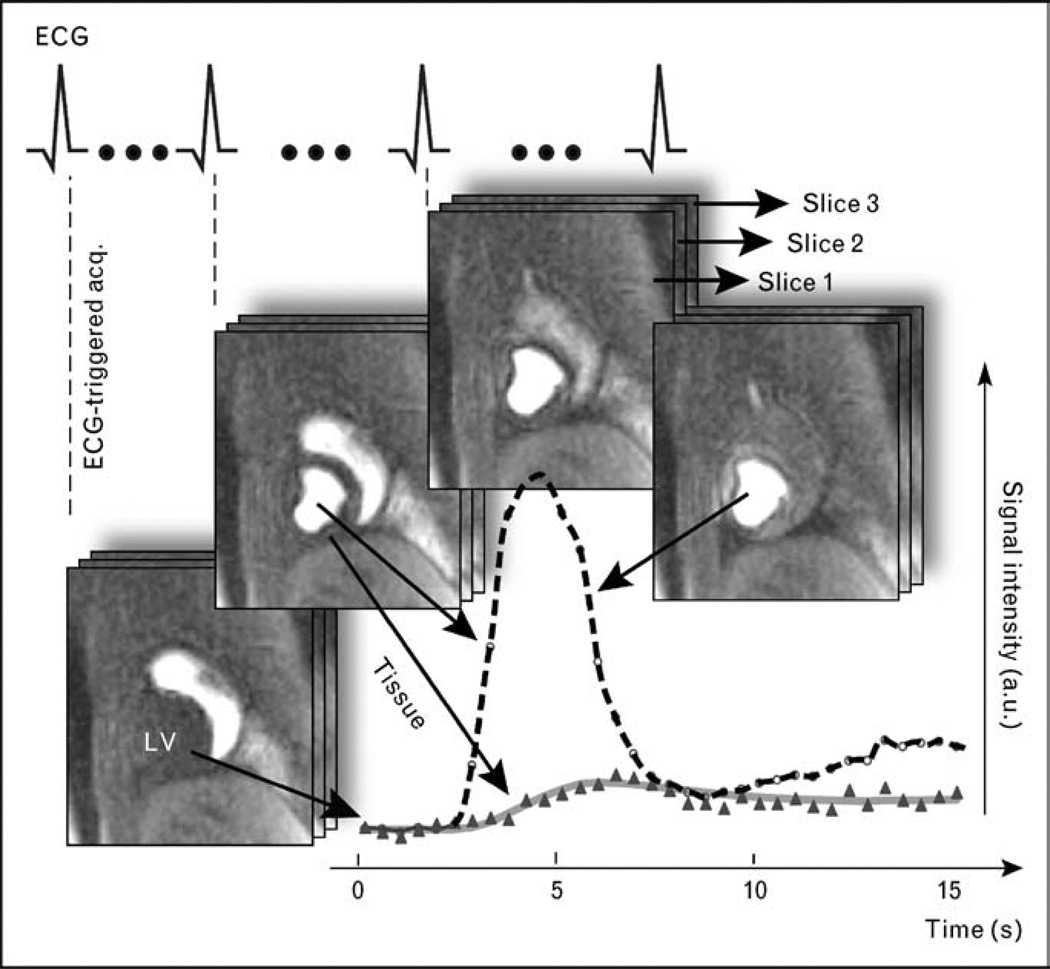
Purpose of review: This review is meant as a balanced summary of the current state of cardiac magnetic resonance (CMR) perfusion imaging in assessing alterations in myocardial blood flow due to coronary artery disease (CAD). We aim to provide first an accessible technical overview of first-pass CMR perfusion imaging and contrast it with other conventional perfusion imaging modalities, and then address the potential advantages of CMR for a qualitative assessment of perfusion defects, as well as quantitative blood flow measurements. Most recent results from clinical trials on the utility of CMR perfusion and novel directions will be explored.
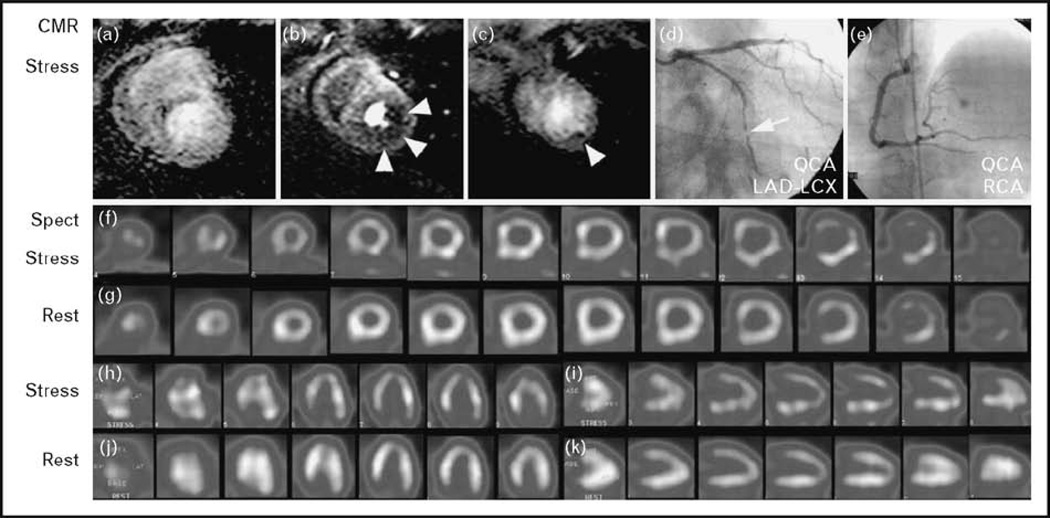
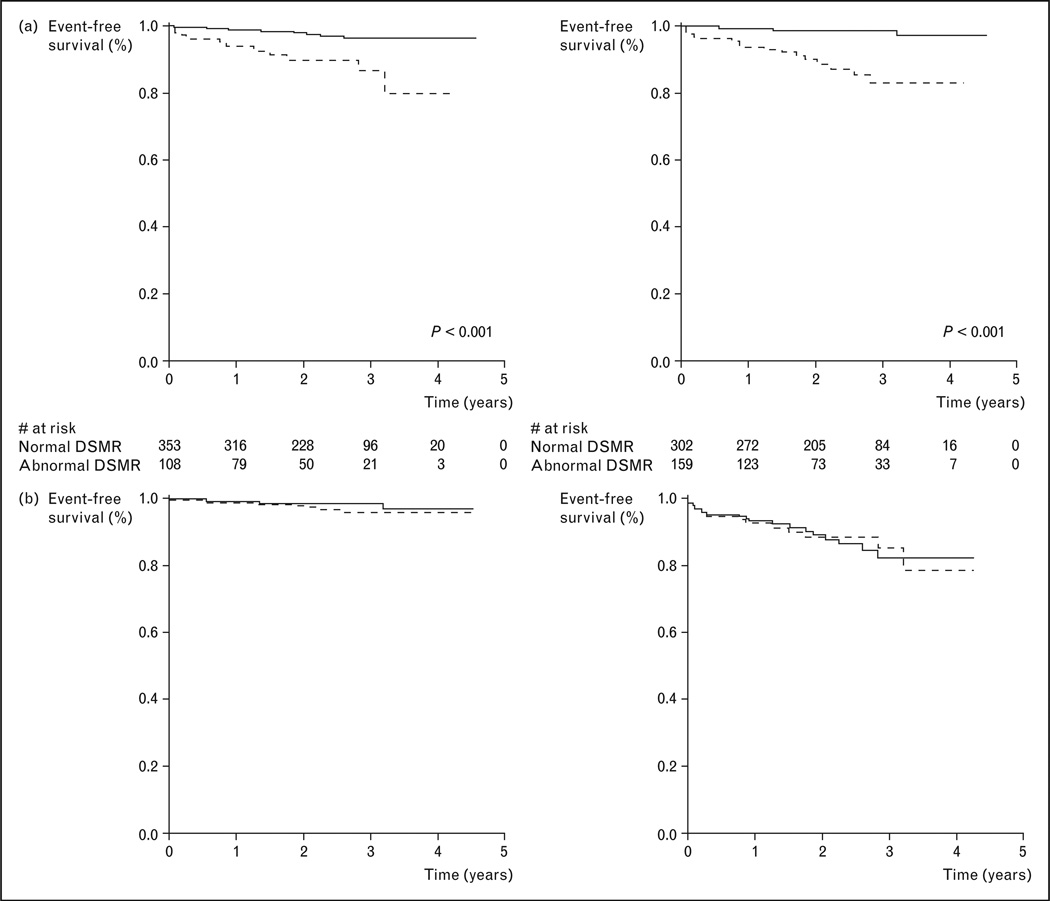
Recent findings: Recent results of the first multicenter multivendor CMR perfusion study demonstrated superior diagnostic utility in detecting CAD by CMR compared with conventional nuclear single-photon emission computed tomography. Several large clinical trials provide additional evidence indicating the strong prognostic implications when CMR perfusion was performed in a clinical setting in patients with an intermediate clinical likelihood of CAD. A negative adenosine stress CMR perfusion study conferred a favorable 3-year prognosis towards nonfatal myocardial infarction or cardiac death.
Summary: CMR perfusion imaging during the first pass of gadolinium-based contrast agents has undergone many technical improvements and levels of clinical validation. Rapidly increasing clinical use worldwide over the last years in diagnosing chest pain syndromes supports the role of CMR in a comprehensive and efficient noninvasive assessment of altered myocardial physiology in CAD.
Figures
References
-
- Wischgoll T, Meyer J, Kaimovitz B, et al. A novel method for visualization of entire coronary arterial tree. Ann Biomed Eng. 2007;35:694–710. - PubMed
-
- Fayad ZA, Fuster V, Fallon JT, et al. Noninvasive in vivo human coronary artery lumen and wall imaging using black-blood magnetic resonance imaging. Circulation. 2000;102:506–510. - PubMed
-
- Worthley SG, Helft G, Fayad ZA, et al. Cardiac gated breath-hold black blood MRI of the coronary artery wall: an in vivo and ex vivo comparison. Int J Cardiovasc Imaging. 2001;17:195–201. - PubMed
-
- Maintz D, Ozgun M, Hoffmeier A, et al. Selective coronary artery plaque visualization and differentiation by contrast-enhanced inversion prepared MRI. Eur Heart J. 2006;27:1732–1736. - PubMed
-
- Bassingthwaigthe JB, Raymond GR, Chan JIS. Principles of tracer kinetics. In: Zaret BL, Beller GA, editors. Nuclear cardiology: state of the art and future directions. St. Louis: Mosby-Year Book; 1993. pp. 3–23.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
