

Nutrition: basis for healthy children and mothers in Bangladesh
- PMID: 18831228
- PMCID: PMC2740711
- DOI: 10.3329/jhpn.v26i3.1899
Nutrition: basis for healthy children and mothers in Bangladesh
Abstract
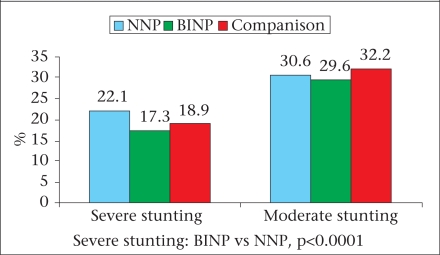
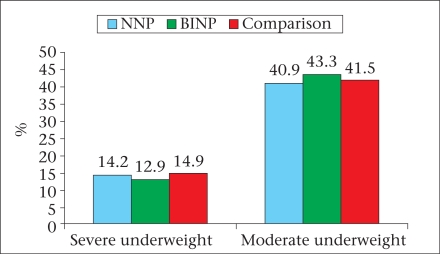
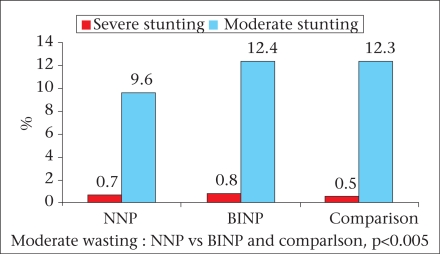
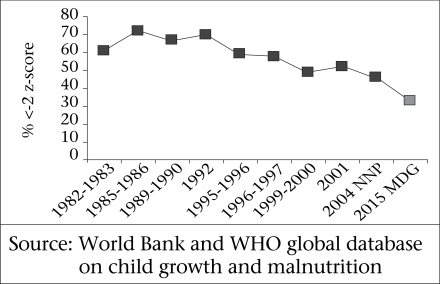
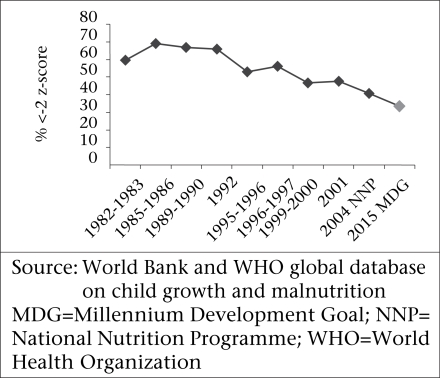
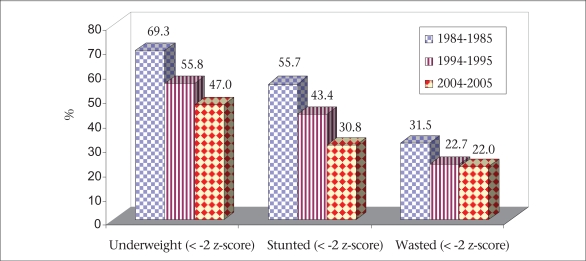
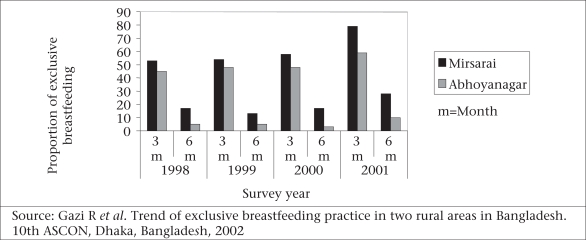
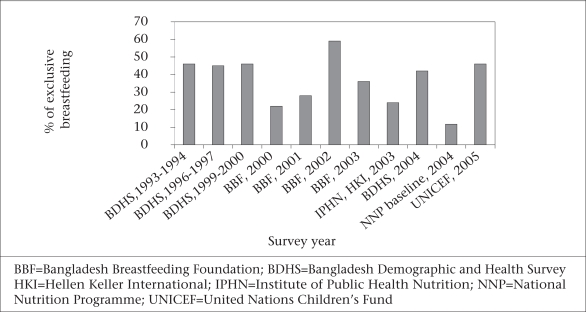
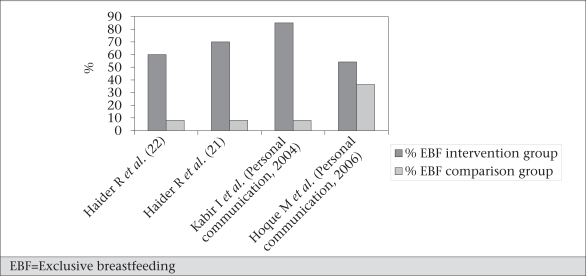
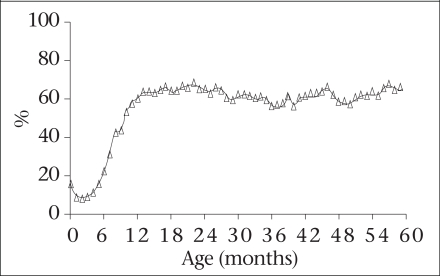
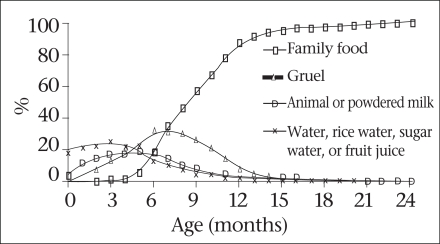
Recent data from the World Health Organization showed that about 60% of all deaths, occurring among children aged less than five years (under-five children) in developing countries, could be attributed to malnutrition. It has been estimated that nearly 50.6 million under-five children are malnourished, and almost 90% of these children are from developing countries. Bangladesh is one of the countries with the highest rate of malnutrition. The recent baseline survey by the National Nutrition Programme (NNP) showed high rates of stunting, underweight, and wasting. However, data from the nutrition surveillance at the ICDDR,B hospital showed that the proportion of children with stunting, underweight, and wasting has actually reduced during 1984-2005. Inappropriate infant and young child-feeding practices (breastfeeding and complementary feeding) have been identified as a major cause of malnutrition. In Bangladesh, although the median duration of breastfeeding is about 30 months, the rate of exclusive breastfeeding until the first six months of life is low, and practice of appropriate complementary feeding is not satisfactory. Different surveys done by the Bangladesh Demographic and Health Survey, United Nations Children's Fund (UNICEF), and Bangladesh Breastfeeding Foundation (BBF) showed a rate of exclusive breastfeeding to be around 32-52%, which have actually remained same or declined over time. The NNP baseline survey using a strict definition of exclusive breastfeeding showed a rate of exclusive breastfeeding (12.8%) until six months of age. Another study from the Abhoynagar field site of ICDDR,B reported the prevalence of exclusive breastfeeding to be 15% only. Considerable efforts have been made to improve the rates of exclusive breastfeeding. Nationally, initiation of breastfeeding within one hour of birth, feeding colostrum, and exclusive breastfeeding have been promoted through the Baby-Friendly Hospital Initiative (BFHI) implemented and supported by BBF and UNICEF respectively. Since most (87-91%) deliveries take place in home, the BFHI has a limited impact on the breastfeeding practices. Results of a few studies done at ICDDR,B and elsewhere in developing countries showed that the breastfeeding peer-counselling method could substantially increase the rates of exclusive breastfeeding. Results of a study in urban Dhaka showed that the rate of exclusive breastfeeding was 70% among mothers who were counselled compared to only 6% who were not counselled. Results of another study in rural Bangladesh showed that peer-counselling given either individually or in a group improved the rate of exclusive breastfeeding from 89% to 81% compared to those mothers who received regular health messages only. This implies that scaling up peer-counselling methods and incorporation of breastfeeding counselling in the existing maternal and child heath programme is needed to achieve the Millennium Development Goal of improving child survival. The recent data showed that the prevalence of starting complementary food among infants aged 6-9 months had increased substantially with 76% in the current dataset. However, the adequacy, frequency, and energy density of the complementary food are in question. Remarkable advances have been made in the hospital management of severely-malnourished children. The protocolized management of severe protein-energy malnutrition at the Dhaka hospital of ICDDR,B has reduced the rate of hospital mortality by 50%. A recent study at ICDDR,B has also documented that home-based management of severe protein-energy malnutrition without follow-up was comparable with a hospital-based protocolized management. Although the community nutrition centres of the NNP have been providing food supplementation and performing growth monitoring of children with protein-energy malnutrition, the referral system and management of complicated severely-malnourished children are still not in place.
Figures
References
-
- Ahmed T, Ali M, Ullah MM, Choudhury IA, Haque ME, Salam MA, et al. Mortality in severely malnourished children with diarrhoea and use of a standardised management protocol. Lancet. 1999;353:1919–22. - PubMed
-
- Pelletier DL, Frongillo EA, Jr., Schroeder DG, Habicht JP. A methodology for estimating the contribution of malnutrition to child mortality in developing countries. J Nutr. 1994;124(Suppl 10):2106S–22S. - PubMed
-
- Murray CJ, Lopez AD. Global mortality, disability, and the contribution of risk factors: Global Burden of Disease Study. Lancet. 1997;349:1436–42. - PubMed
-
- State of the world's children. New York, NY: United Nations Children's Fund; 2002. United Nations Children's Fund; p. 103.
-
- Richardson SA. The relation of severe malnutrition in infancy to the intelligence of school children with differing life histories. Pediatr Res. 1976;10:57–61. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical