

Bezoar in gastro-jejunostomy presenting with symptoms of gastric outlet obstruction: a case report and review of the literature
- PMID: 18831730
- PMCID: PMC2567335
- DOI: 10.1186/1752-1947-2-323
Bezoar in gastro-jejunostomy presenting with symptoms of gastric outlet obstruction: a case report and review of the literature
Abstract
Introduction: Gastric outlet obstruction usually presents with non-bilious vomiting, colicky epigastric pain, loss of appetite and occasionally, upper gastrointestinal bleeding. Causes can be classified as benign or malignant, or as extra- or intraluminal. Gastrojejunostomy is a well-recognised surgical procedure performed to bypass gastric outlet obstruction. A bezoar occurs most commonly in patients with impaired gastrointestinal motility or with a history of gastric surgery. It is an intestinal concretion, which fails to pass along the alimentary canal.
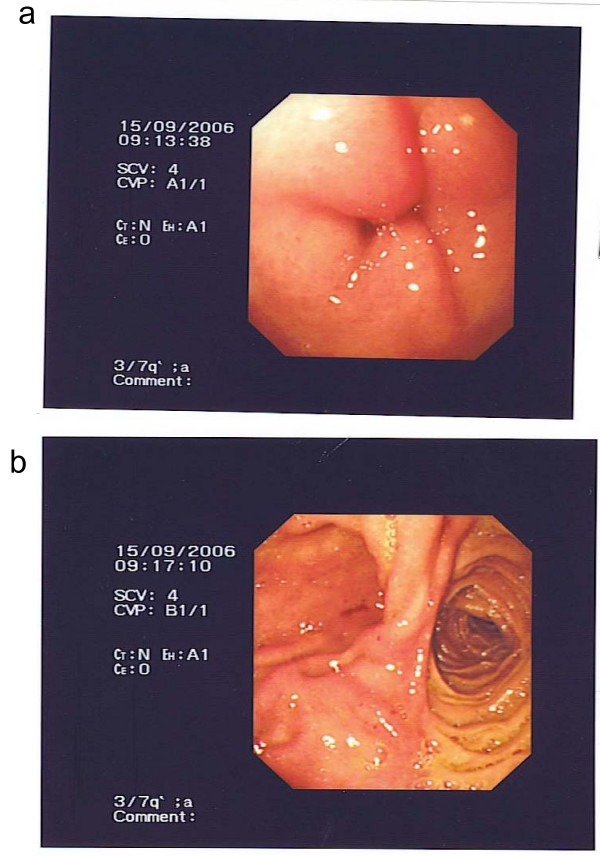
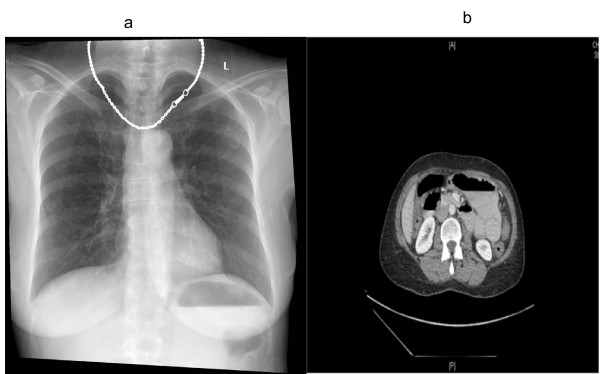
Case presentation: A 62-year-old Asian woman with a history of gastrojejunostomy for peptic ulcer disease was admitted to hospital with epigastric pain, vomiting and dehydration. All investigations concluded gastric outlet obstruction secondary to a "stricture" at the site of gastrojejunostomy. Subsequent laparotomy revealed that the cause of the obstruction was a bezoar.
Conclusion: Many bezoars can be removed endoscopically, but some will require operative intervention. Once removed, emphasis must be placed upon prevention of recurrence. Surgeons must learn to recognise and classify bezoars in order to provide the most effective therapy.
Figures

References
LinkOut - more resources
Full Text Sources
