

Patterns of skeletal fractures in child abuse: systematic review
- PMID: 18832412
- PMCID: PMC2563260
- DOI: 10.1136/bmj.a1518
Patterns of skeletal fractures in child abuse: systematic review
Abstract
Objectives: To systematically review published studies to identify the characteristics that distinguish fractures in children resulting from abuse and those not resulting from abuse, and to calculate a probability of abuse for individual fracture types.
Design: Systematic review.
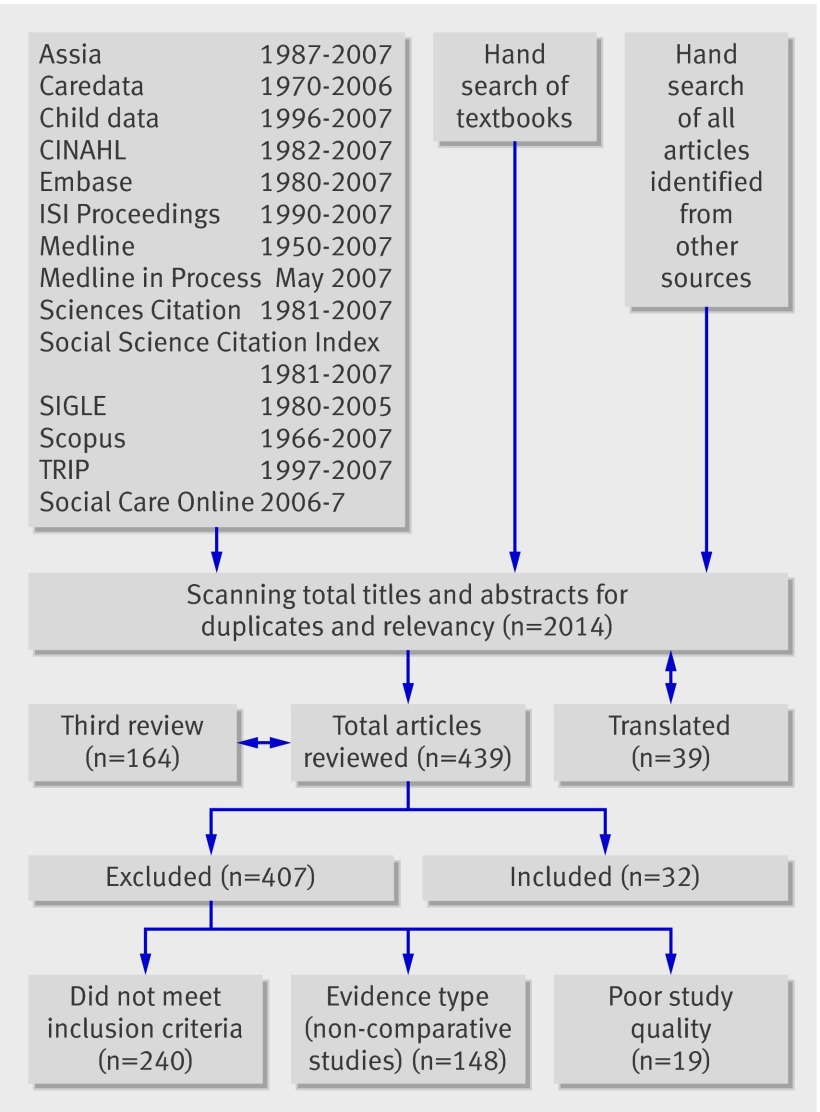
Data sources: All language literature search of Medline, Medline in Process, Embase, Assia, Caredata, Child Data, CINAHL, ISI Proceedings, Sciences Citation, Social Science Citation Index, SIGLE, Scopus, TRIP, and Social Care Online for original study articles, references, textbooks, and conference abstracts until May 2007.
Study selection: Comparative studies of fracture at different bony sites, sustained in physical abuse and from other causes in children <18 years old were included. Review articles, expert opinion, postmortem studies, and studies in adults were excluded. Data extraction and synthesis Each study had two independent reviews (three if disputed) by specialist reviewers including paediatricians, paediatric radiologists, orthopaedic surgeons, and named nurses in child protection. Each study was critically appraised by using data extraction sheets, critical appraisal forms, and evidence sheets based on NHS Centre for Reviews and Dissemination guidance. Meta-analysis was done where possible. A random effects model was fitted to account for the heterogeneity between studies.
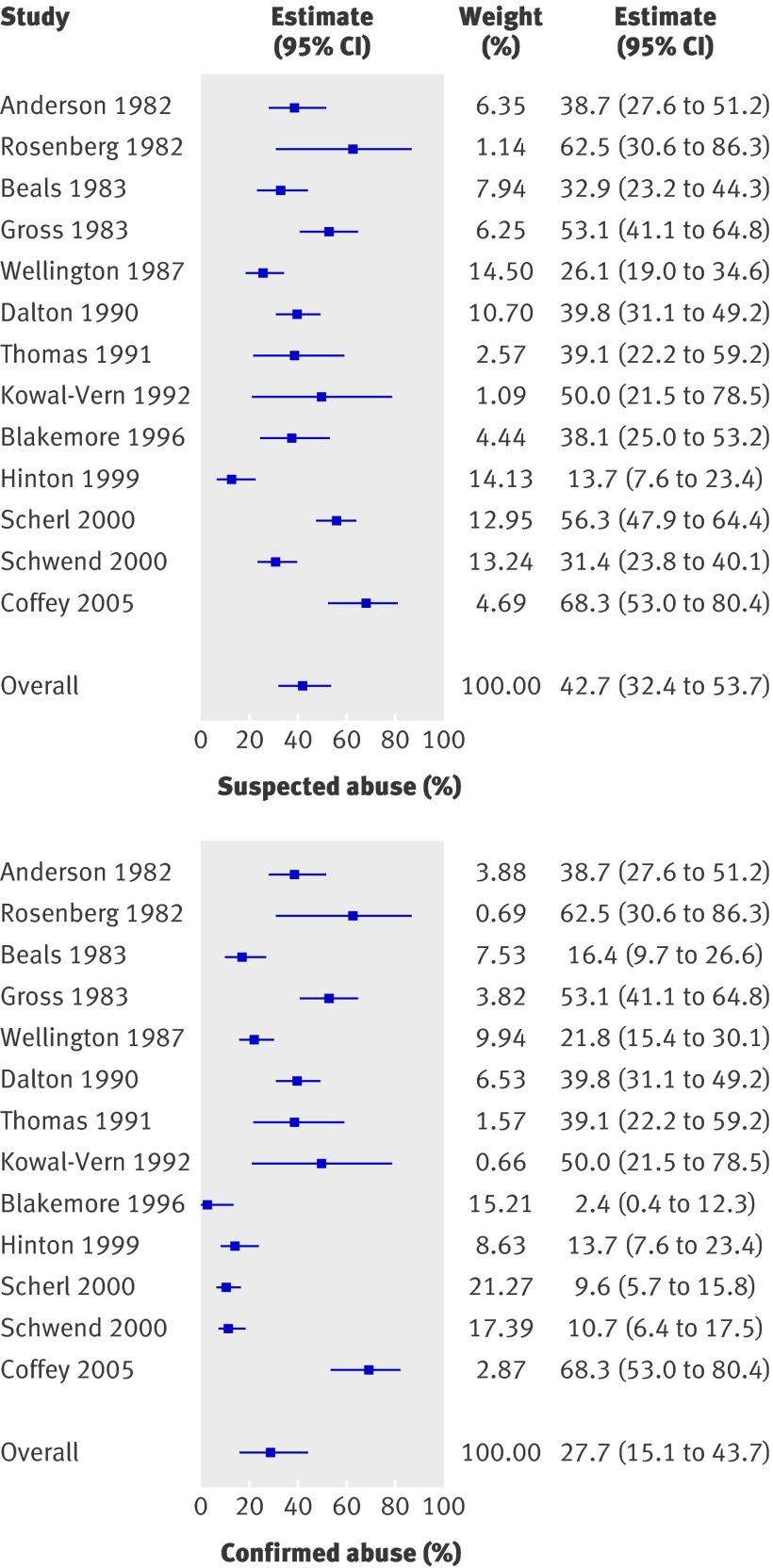
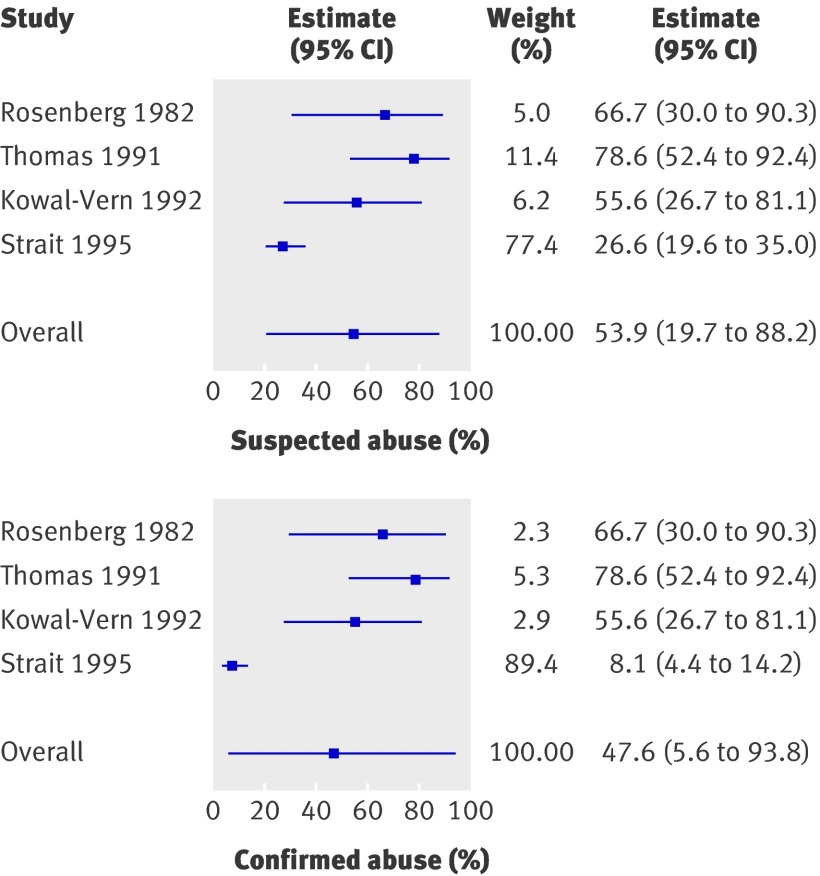
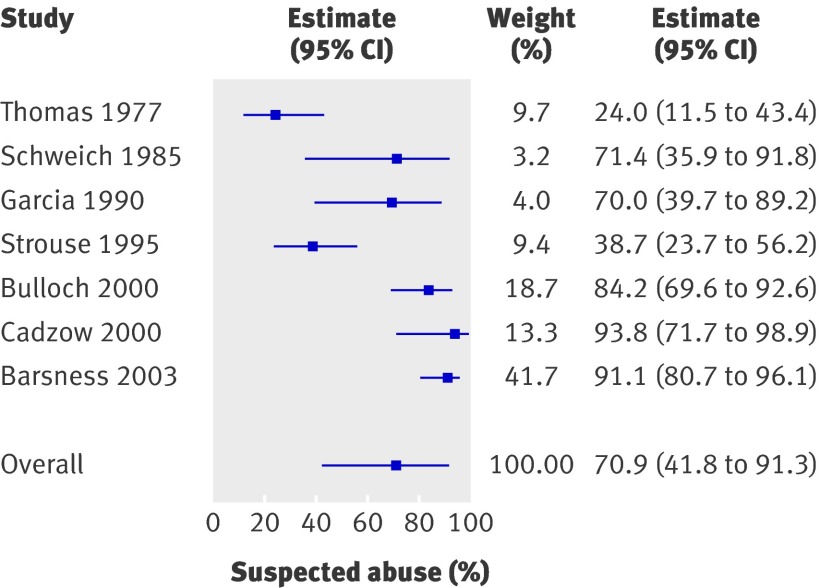
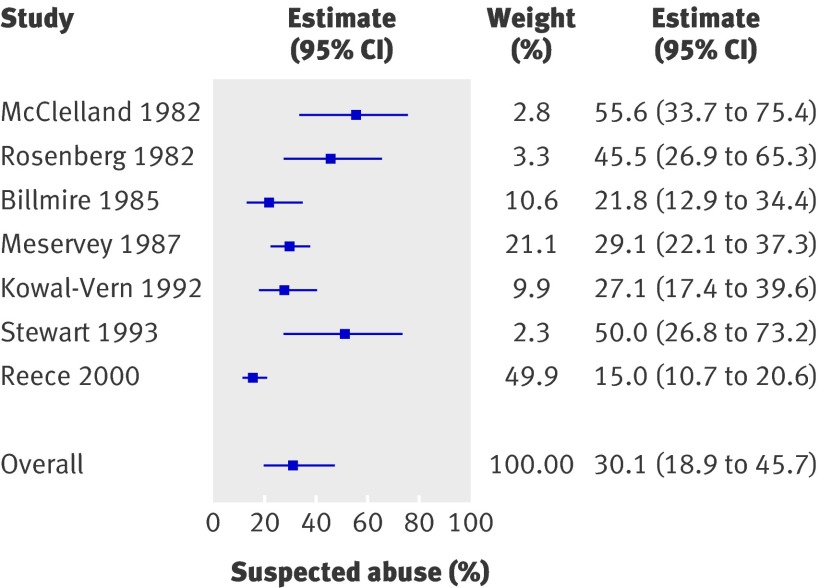
Results: In total, 32 studies were included. Fractures resulting from abuse were recorded throughout the skeletal system, most commonly in infants (<1 year) and toddlers (between 1 and 3 years old). Multiple fractures were more common in cases of abuse. Once major trauma was excluded, rib fractures had the highest probability for abuse (0.71, 95% confidence interval 0.42 to 0.91). The probability of abuse given a humeral fracture lay between 0.48 (0.06 to 0.94) and 0.54 (0.20 to 0.88), depending on the definition of abuse used. Analysis of fracture type showed that supracondylar humeral fractures were less likely to be inflicted. For femoral fractures, the probability was between 0.28 (0.15 to 0.44) and 0.43 (0.32 to 0.54), depending on the definition of abuse used, and the developmental stage of the child was an important discriminator. The probability for skull fractures was 0.30 (0.19 to 0.46); the most common fractures in abuse and non-abuse were linear fractures. Insufficient comparative studies were available to allow calculation of a probability of abuse for other fracture types.
Conclusion: When infants and toddlers present with a fracture in the absence of a confirmed cause, physical abuse should be considered as a potential cause. No fracture, on its own, can distinguish an abusive from a non-abusive cause. During the assessment of individual fractures, the site, fracture type, and developmental stage of the child can help to determine the likelihood of abuse. The number of high quality comparative research studies in this field is limited, and further prospective epidemiology is indicated.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Diagnosing child abuse.BMJ. 2008 Oct 2;337:a1398. doi: 10.1136/bmj.a1398. BMJ. 2008. PMID: 18832411 No abstract available.
-
Patterns of skeletal fractures in child abuse. "Unexplained" fractures.BMJ. 2008 Oct 28;337:a2279. doi: 10.1136/bmj.a2279. BMJ. 2008. PMID: 18957460 No abstract available.
References
-
- Merten DF, Radlowski MA, Leonidas JC. The abused child: a radiological reappraisal. Radiology 1983;146:377-81. - PubMed
-
- Feldman KW, Brewer DK. Child abuse, cardiopulmonary resuscitation and rib fractures. Pediatrics 1984;73:339-42. - PubMed
-
- Belfer RA, Klein BL, Orr L. Use of the skeletal survey in the evaluation of child maltreatment. Am J Emerg Med 2001;19:122-4. - PubMed
-
- Day F, Clegg S, McPhillips M, Mok J. A retrospective case series of skeletal surveys in children with suspected non-accidental injury. J Clin Forensic Med 2006;13:55-9. - PubMed
-
- Rennie L, Court-Brown CM, Mok JY, Beattie TF. The epidemiology of fractures in children. Injury 2007;38:913-22. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical