

A biomarker panel for acute graft-versus-host disease
- PMID: 18832652
- PMCID: PMC2615645
- DOI: 10.1182/blood-2008-07-167098
A biomarker panel for acute graft-versus-host disease
Abstract
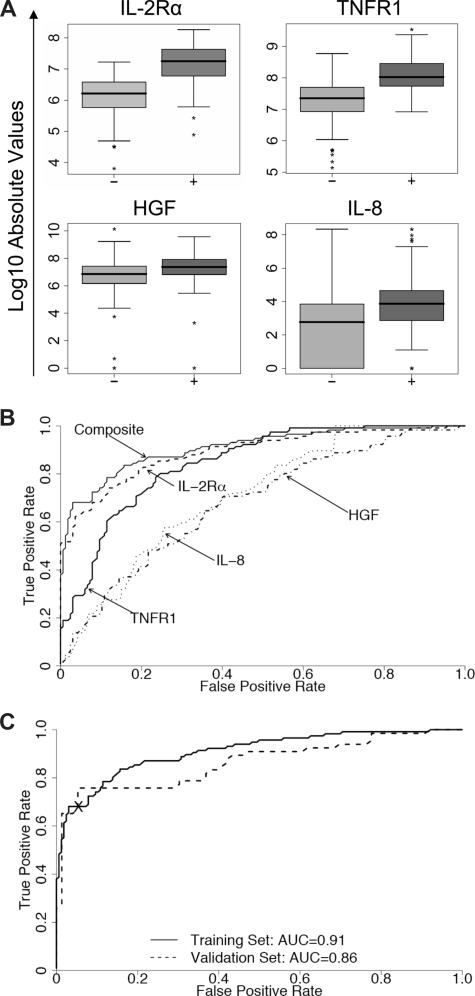
No validated biomarkers exist for acute graft-versus-host disease (GVHD). We screened plasma with antibody microarrays for 120 proteins in a discovery set of 42 patients who underwent transplantation that revealed 8 potential biomarkers for diagnostic of GVHD. We then measured by enzyme-linked immunosorbent assay (ELISA) the levels of these biomarkers in samples from 424 patients who underwent transplantation randomly divided into training (n = 282) and validation (n = 142) sets. Logistic regression analysis of these 8 proteins determined a composite biomarker panel of 4 proteins (interleukin-2-receptor-alpha, tumor-necrosis-factor-receptor-1, interleukin-8, and hepatocyte growth factor) that optimally discriminated patients with and without GVHD. The area under the receiver operating characteristic curve distinguishing these 2 groups in the training set was 0.91 (95% confidence interval, 0.87-0.94) and 0.86 (95% confidence interval, 0.79-0.92) in the validation set. In patients with GVHD, Cox regression analysis revealed that the biomarker panel predicted survival independently of GVHD severity. A panel of 4 biomarkers can confirm the diagnosis of GVHD in patients at onset of clinical symptoms of GVHD and provide prognostic information independent of GVHD severity.
Figures


Comment in
-
Graft-versus-host disease: proteomics comes of age.Blood. 2009 Jan 8;113(2):271-2. doi: 10.1182/blood-2008-10-185991. Blood. 2009. PMID: 19131558 No abstract available.
References
-
- Przepiorka D, Weisdorf D, Martin P, et al. 1994 Consensus Conference on Acute GVHD Grading. Bone Marrow Transplant. 1995;15:825–828. - PubMed
-
- Martin PJ, Schoch G, Fisher L, et al. A retrospective analysis of therapy for acute graft-versus-host disease: secondary treatment. Blood. 1991;77:1821–1828. - PubMed
-
- Miyamoto T, Akashi K, Hayashi S, et al. Serum concentration of the soluble interleukin-2 receptor for monitoring acute graft-versus-host disease. Bone Marrow Transplant. 1996;17:185–190. - PubMed
-
- Grimm J, Zeller W, Zander AR. Soluble interleukin-2 receptor serum levels after allogeneic bone marrow transplantations as a marker for GVHD. Bone Marrow Transplant. 1998;21:29–32. - PubMed
-
- Foley R, Couban S, Walker I, et al. Monitoring soluble interleukin-2 receptor levels in related and unrelated donor allogenic bone marrow transplantation. Bone Marrow Transplant. 1998;21:769–773. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
