

A comparison of clinical and immunologic features in children and older patients hospitalized with severe cholera in Bangladesh
- PMID: 18833030
- PMCID: PMC2749325
- DOI: 10.1097/INF.0b013e3181783adf
A comparison of clinical and immunologic features in children and older patients hospitalized with severe cholera in Bangladesh
Abstract
Background: : Infection with Vibrio cholerae induces protection from subsequent severe disease, suggesting that an effective vaccine could be an important preventive strategy. Available vaccines provide less protection against cholera than natural infection, particularly in children.
Methods: : We examined a cohort of 121 children (2 years-12 years of age) and 276 older patients (>12 years of age) hospitalized with cholera in Dhaka, Bangladesh over a 4-year period, to compare clinical features in older patients and children and immune responses to key antigens.
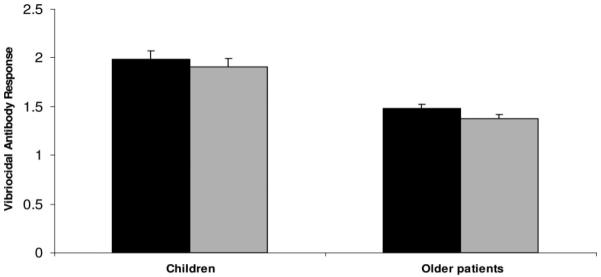
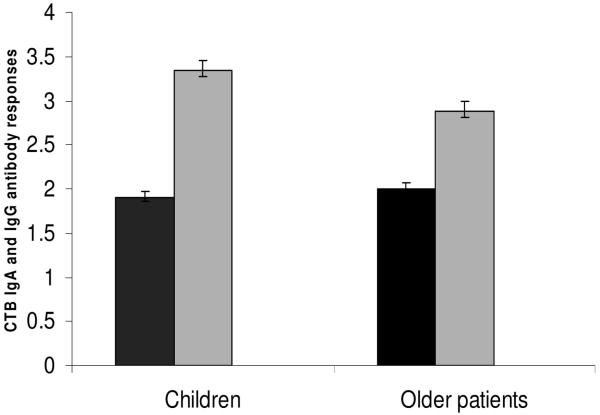
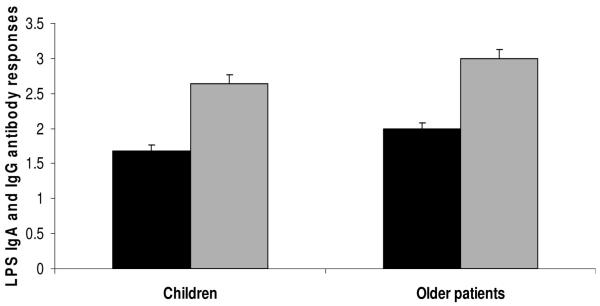
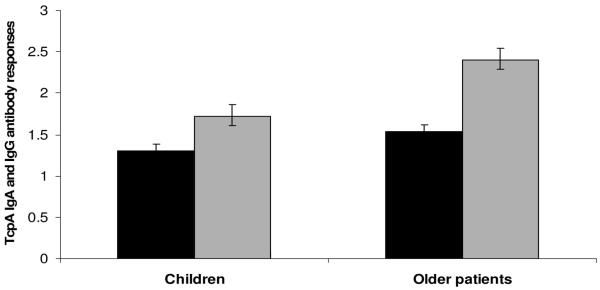
Results: : Older patients had more severe disease. Children with cholera were more commonly retinol deficient, while zinc deficiency was equally prevalent in both groups. Children developed higher vibriocidal and serum immune responses to the B subunit of cholera toxin (CTB). In contrast, older patients mounted higher immune responses to 2 other key V. cholerae antigens, the lipopolysaccharide (LPS) and toxin coregulated pilus antigens (TcpA). We compared immune responses following infection with those occurring after receipt of a live, oral vaccine in both children and older patients in Bangladesh, during a similar time period. The response rates for vibriocidal and LPS antibodies were higher after infection than after vaccination. Both vaccinated older patients and children responded poorly to CTB and TcpA.
Conclusions: : Although children developed vigorous vibriocidal and CTB-specific responses following infection, they had lessened responses to LPS and TcpA compared with older patients, as well as lessened responses to vaccination. More studies need to be carried out to determine factors, including micronutrient interventions that can improve responses in children to both natural infection and vaccination.
Figures
References
-
- Cholera Working Group. International Centre for Diarrhoeal Diseases Research Large epidemic of cholera-like disease in Bangladesh caused by Vibrio cholerae O139 synonym Bengal. Lancet. 1993;342:387–390. Bangladesh. - PubMed
-
- Sack RB, Siddique AK, Longini IM, Jr, et al. A 4-year study of the epidemiology of Vibrio cholerae in four rural areas of Bangladesh. J Infect Dis. 2003;187:96–101. - PubMed
-
- Albert MJ. Epidemiology & molecular biology of Vibrio cholerae O139 Bengal. Indian J Med Res. 1996;104:14–27. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
