

Polymicrobial nature of chronic diabetic foot ulcer biofilm infections determined using bacterial tag encoded FLX amplicon pyrosequencing (bTEFAP)
- PMID: 18833331
- PMCID: PMC2556099
- DOI: 10.1371/journal.pone.0003326
Polymicrobial nature of chronic diabetic foot ulcer biofilm infections determined using bacterial tag encoded FLX amplicon pyrosequencing (bTEFAP)
Abstract
Background: Diabetic extremity ulcers are associated with chronic infections. Such ulcer infections are too often followed by amputation because there is little or no understanding of the ecology of such infections or how to control or eliminate this type of chronic infection. A primary impediment to the healing of chronic wounds is biofilm phenotype infections. Diabetic foot ulcers are the most common, disabling, and costly complications of diabetes. Here we seek to derive a better understanding of the polymicrobial nature of chronic diabetic extremity ulcer infections.
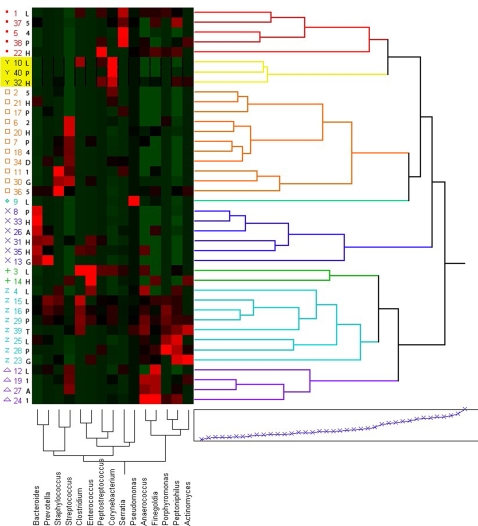
Methods and findings: Using a new bacterial tag encoded FLX amplicon pyrosequencing (bTEFAP) approach we have evaluated the bacterial diversity of 40 chronic diabetic foot ulcers from different patients. The most prevalent bacterial genus associated with diabetic chronic wounds was Corynebacterium spp. Findings also show that obligate anaerobes including Bacteroides, Peptoniphilus, Fingoldia, Anaerococcus, and Peptostreptococcus spp. are ubiquitous in diabetic ulcers, comprising a significant portion of the wound biofilm communities. Other major components of the bacterial communities included commonly cultured genera such as Streptococcus, Serratia, Staphylococcus and Enterococcus spp.
Conclusions: In this article, we highlight the patterns of population diversity observed in the samples and introduce preliminary evidence to support the concept of functional equivalent pathogroups (FEP). Here we introduce FEP as consortia of genotypically distinct bacteria that symbiotically produce a pathogenic community. According to this hypothesis, individual members of these communities when they occur alone may not cause disease but when they coaggregate or consort together into a FEP the synergistic effect provides the functional equivalence of well-known pathogens, such as Staphylococcus aureus, giving the biofilm community the factors necessary to maintain chronic biofilm infections. Further work is definitely warranted and needed in order to prove whether the FEPs concept is a viable hypothesis. The findings here also suggest that traditional culturing methods may be extremely biased as a diagnostic tool as they select for easily cultured organisms such as Staphylococcus aureus and against difficult to culture bacteria such as anaerobes. While PCR methods also have bias, further work is now needed in comparing traditional culture results to high-resolution molecular diagnostic methods such as bTEFAP.
Conflict of interest statement
Figures
References
-
- Costerton JW, Lewandowski Z, Caldwell DE, Korber DR, Lappin-Scott HM. Microbial biofilms. Annu Rev Microbiol. 1995;49:711–745. - PubMed
-
- Smith A. Etiology of the Problem Wound. In: Sheffield PJ, Fife CE, Smith A, editors. Wound Care Practice. Flagstaff: Best Publishing Company; 2004. pp. 3–48.
-
- CDCDFWC. Consensus Development Conference on Diabetic Foot Wound Care: 7–8 April 1999, Boston, Massachusetts. American Diabetes Association. Diabetes Care. 1999;22:1354–1360. - PubMed
-
- Palumbo PJ, Melton LJI. Diabetes in America: diabetes data compiled 1984. Washington, D.C: Government Printing Office; 1985. Peripheral vascular disease and diabetes.
-
- Adler AI, Boyko EJ, Ahroni JH, Smith DG. Lower-extremity amputation in diabetes. The independent effects of peripheral vascular disease, sensory neuropathy, and foot ulcers. Diabetes Care. 1999;22:1029–1035. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
