

Hepatitis B and hepatitis C in Pakistan: prevalence and risk factors
- PMID: 18835208
- PMCID: PMC2651958
- DOI: 10.1016/j.ijid.2008.06.019
Hepatitis B and hepatitis C in Pakistan: prevalence and risk factors
Abstract
Background: Pakistan carries one of the world's highest burdens of chronic hepatitis and mortality due to liver failure and hepatocellular carcinomas. However, national level estimates of the prevalence of and risk factors for hepatitis B and hepatitis C are currently not available.
Methods: We reviewed the medical and public health literature over a 13-year period (January 1994-September 2007) to estimate the prevalence of active hepatitis B and chronic hepatitis C in Pakistan, analyzing data separately for the general and high-risk populations and for each of the four provinces. We included 84 publications with 139 studies (42 studies had two or more sub-studies).
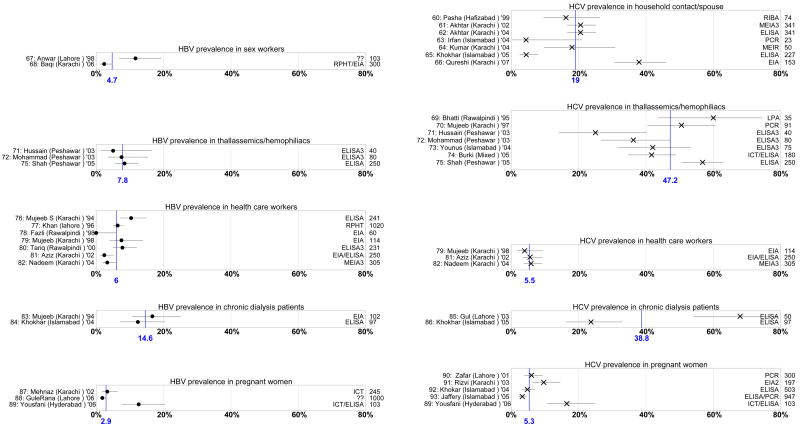
Results: Methodological differences in studies made it inappropriate to conduct a formal meta-analysis to determine accurate national prevalence estimates, but we estimated the likely range of prevalence in different population sub-groups. A weighted average of hepatitis B antigen prevalence in pediatric populations was 2.4% (range 1.7-5.5%) and for hepatitis C antibody was 2.1% (range 0.4-5.4%). A weighted average of hepatitis B antigen prevalence among healthy adults (blood donors and non-donors) was 2.4% (range 1.4-11.0%) and for hepatitis C antibody was 3.0% (range 0.3-31.9%). Rates in the high-risk subgroups were far higher.
Conclusions: Data suggest a moderate to high prevalence of hepatitis B and hepatitis C in different areas of Pakistan. The published literature on the modes of transmission of hepatitis B and hepatitis C in Pakistan implicate contaminated needle use in medical care and drug abuse and unsafe blood and blood product transfusion as the major causal factors.
Conflict of interest statement
Figures


References
-
- Previsani N, Lavanchy D. WHO/CDS/CSR/LYO/2002.2:Hepatitis B. Geneva: World Health Organization; 2002. Hepatitis B.
-
- Hepatitis C. Geneva: World Health Organization; 2000. [(accessed August 2008 [Au?3]]. World Health Organization fact sheets. Available at: http://www.who.int/mediacentre/factsheets/fs164/en/
-
- Perz JF, Armstrong GL, Farrington LA, Hutin YJ, Bell BP. The contributions of hepatitis B virus and hepatitis C virus infections to cirrhosis and primary liver cancer worldwide. J Hepatol. 2006;45:529–38. - PubMed
-
- The world factbook. Pakistan. USA: Central Intelligence Agency. 2007. [accessed August 2008]. Available at: https://www.cia.gov/library/publications/the-world-factbook/geos/pk.html [Au?4]
-
- California state facts. United States Geological Survey. 2006. [accessed August 2008]. Available at: http://www.usgs.gov.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
