

Prediagnostic body-mass index, plasma C-peptide concentration, and prostate cancer-specific mortality in men with prostate cancer: a long-term survival analysis
- PMID: 18835745
- PMCID: PMC2651222
- DOI: 10.1016/S1470-2045(08)70235-3
Prediagnostic body-mass index, plasma C-peptide concentration, and prostate cancer-specific mortality in men with prostate cancer: a long-term survival analysis
Abstract
Background: Excess body-mass index (BMI) has been associated with adverse outcomes in prostate cancer, and hyperinsulinaemia is a candidate mediator, but prospective data are sparse. We assessed the effect of prediagnostic BMI and plasma C-peptide concentration (reflecting insulin secretion) on prostate cancer-specific mortality after diagnosis.
Methods: This study involved men diagnosed with prostate cancer during the 24 years of follow-up in the Physicians' Health Study. BMI measurements were available at baseline in 1982 and eight years later in 1990 for 2546 men who developed prostate cancer. Baseline C-peptide concentration was available in 827 men. We used Cox proportional hazards regression models controlling for age, smoking, time between BMI measurement and prostate cancer diagnosis, and competing causes of death to assess the risk of prostate cancer-specific mortality according to BMI and C-peptide concentration.
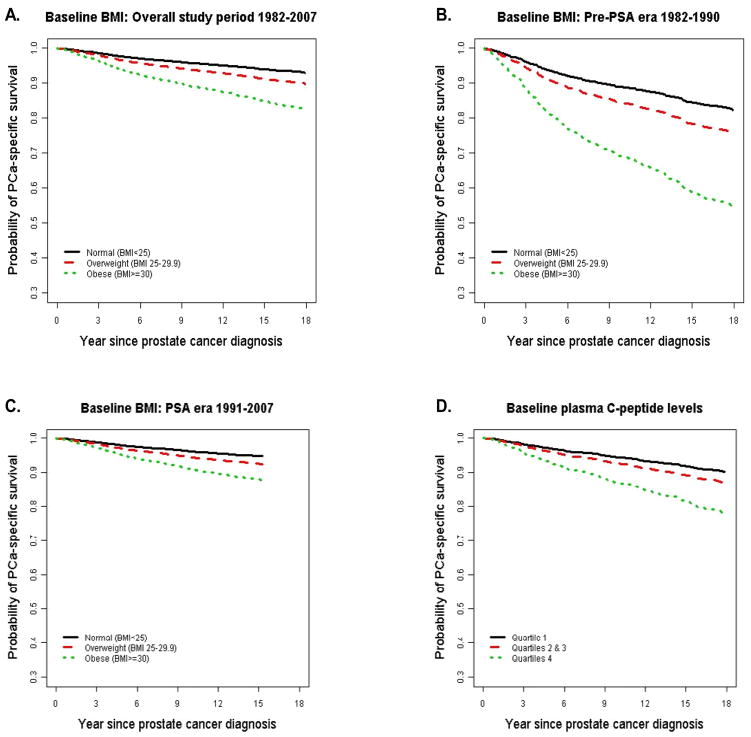
Findings: Of the 2546 men diagnosed with prostate cancer during the follow-up period, 989 (38.8%) were overweight (BMI 25.0-29.9 kg/m(2)) and 87 (3.4%) were obese (BMI >/=30 kg/m(2)). 281 men (11%) died from prostate cancer during this follow-up period. Compared with men of a healthy weight (BMI <25 kg/m(2)) at baseline, overweight men and obese men had a significantly higher risk of prostate cancer mortality (proportional hazard ratio [HR] 1.47 [95% CI 1.16-1.88] for overweight men and 2.66 [1.62-4.39] for obese men; p(trend)<0.0001). The trend remained significant after controlling for clinical stage and Gleason grade and was stronger for prostate cancer diagnosed during the PSA screening era (1991-2007) compared with during the pre-PSA screening era (1982-1990) or when using BMI measurements obtained in 1990 compared with those obtained in 1982. Of the 827 men with data available for baseline C-peptide concentration, 117 (14%) died from prostate cancer. Men with C-peptide concentrations in the highest quartile (high) versus the lowest quartile (low) had a higher risk of prostate cancer mortality (HR 2.38 [95% CI 1.31-4.30]; p(trend)=0.008). Compared with men with a BMI less than 25 kg/m(2) and low C-peptide concentrations, those with a BMI of 25 kg/m(2) or more and high C-peptide concentrations had a four-times higher risk of mortality (4.12 [1.97-8.61]; p(interaction)=0.001) independent of clinical predictors.
Interpretation: Excess bodyweight and a high plasma concentration of C-peptide both predispose men with a subsequent diagnosis of prostate cancer to an increased likelihood of dying of their disease. Patients with both factors have the worst outcome. Further studies are now needed to confirm these findings.
Conflict of interest statement
Conflict of Interest Statement
The authors state no conflict of interest.
Figures
Comment in
-
Prostate cancer and host metabolic factors.Lancet Oncol. 2008 Nov;9(11):1022-3. doi: 10.1016/S1470-2045(08)70265-1. Lancet Oncol. 2008. PMID: 19012851 No abstract available.
References
-
- MacInnis RJ, English DR. Body size and composition and prostate cancer risk: systematic review and meta-regression analysis. Cancer Causes Control. 2006 Oct;17(8):989–1003. - PubMed
-
- Littman AJ, White E, Kristal AR. Anthropometrics and prostate cancer risk. Am J Epidemiol. 2007 Jun 1;165(11):1271–9. - PubMed
-
- Rodriguez C, Freedland SJ, Deka A, et al. Body mass index, weight change, and risk of prostate cancer in the Cancer Prevention Study II Nutrition Cohort. Cancer Epidemiol Biomarkers Prev. 2007 Jan;16(1):63–9. - PubMed
-
- Wright ME, Chang SC, Schatzkin A, et al. Prospective study of adiposity and weight change in relation to prostate cancer incidence and mortality. Cancer. 2007 Feb 15;109(4):675–84. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- P30 DK040561/DK/NIDDK NIH HHS/United States
- R29 CA078293/CA/NCI NIH HHS/United States
- R01 CA090598/CA/NCI NIH HHS/United States
- R01 HL034595/HL/NHLBI NIH HHS/United States
- CA90598/CA/NCI NIH HHS/United States
- CA58684/CA/NCI NIH HHS/United States
- R01 CA058684/CA/NCI NIH HHS/United States
- CA42182/CA/NCI NIH HHS/United States
- R01 CA040360/CA/NCI NIH HHS/United States
- R01 CA034944/CA/NCI NIH HHS/United States
- R01 CA042182/CA/NCI NIH HHS/United States
- R01 HL026490/HL/NHLBI NIH HHS/United States
- R01 CA097193/CA/NCI NIH HHS/United States
- CA40360/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
