

Plasmacytoid dendritic cells are proportionally expanded at diagnosis of type 1 diabetes and enhance islet autoantigen presentation to T-cells through immune complex capture
- PMID: 18835928
- PMCID: PMC2606862
- DOI: 10.2337/db08-0964
Plasmacytoid dendritic cells are proportionally expanded at diagnosis of type 1 diabetes and enhance islet autoantigen presentation to T-cells through immune complex capture
Abstract
Objective: Immune-mediated destruction of beta-cells resulting in type 1 diabetes involves activation of proinflammatory, islet autoreactive T-cells, a process under the control of dendritic cells of the innate immune system. We tested the hypothesis that type 1 diabetes development is associated with disturbance of blood dendritic cell subsets that could enhance islet-specific autoimmunity.
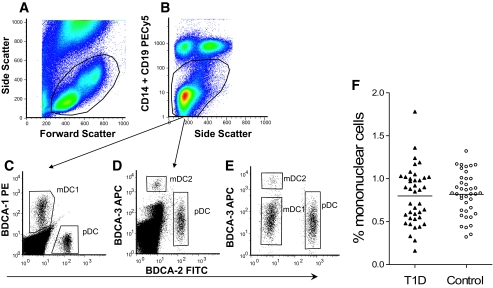
Research design and methods: We examined blood dendritic cells (plasmacytoid and myeloid) in 40 patients with recent-onset diabetes (median duration 28 days) and matched control subjects. We also examined the relative ability of different dendritic cell subsets to process and present soluble or immune complexed islet cell autoantigen (the islet tyrosine phosphatase IA-2) to responder CD4 T-cells.
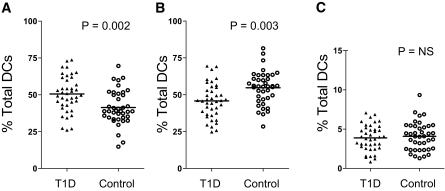
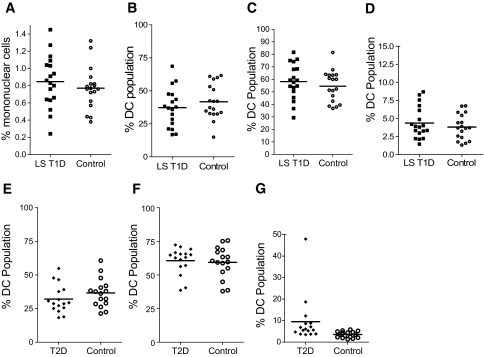
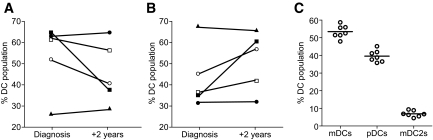
Results: The balance of blood dendritic cells was profoundly disturbed at diabetes diagnosis, with a significantly elevated proportion of plasmacytoid and reduction of myeloid cells compared with control subjects. Dendritic cell subset distribution was normal in long-standing disease and in patients with type 2 diabetes. Both dendritic cell subsets processed and presented soluble IA-2 to CD4 T-cells after short-term culture, but only plasmacytoid dendritic cells enhanced (by as much as 100%) autoantigen presentation in the presence of IA-2(+) autoantibody patient serum.
Conclusions: The plasmacytoid subset of dendritic cells is overrepresented in the blood close to diabetes onset and shows a distinctive ability to capture islet autoantigenic immune complexes and enhance autoantigen-driven CD4 T-cell activation. This suggests a synergistic proinflammatory role for plasmacytoid dendritic cells and islet cell autoantibodies in type 1 diabetes.
Figures
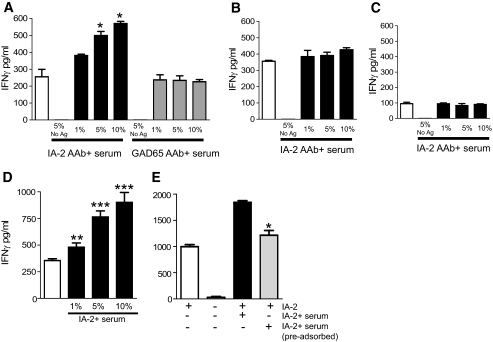
 ; 1–10%) has no effect on presentation. Likewise, pooled AB serum at these concentrations has no effect (data not shown). In the presence of 5% serum but no IA-2ic-HA307–319, there is no T-cell activation. Data represent one of four experiments using four different cell donors. D: Pooled data from a total of four donors (including the one used in A) for plasmacytoid dendritic cell enhancement of IA-2ic-HA307–319 (▪) presentation to JNZ-1 clone cells (*P < 0.05, **P < 0.01, and ***P < 0.001 vs. presence of antigen alone; □). The additional sera contained 3,875.1, 3,263.1, and 3,007.8 WHO units of IA-2 autoantibodies. Bars represent means ± SE from quadruplicate wells of individual experiments. E: IA-2+ serum–enhanced IA-2ic-HA307–319 presentation is dependent on the serum IgG fraction. Serum has been adsorbed using Protein A matrix. Serum IgG level before adsorption, 6.54 g/l; after adsorption, 0.22 g/l. Serum was used at 5% concentration in these experiments. Serum IA-2 autoantibody level before adsorption, 2,152 WHO units; after adsorption, IA-2 autoantibodies were not detectable. *Significant reduction in IFN-γ production by clone JNZ-1 in the presence of adsorbed compared with nonadsorbed serum (P < 0.05).
; 1–10%) has no effect on presentation. Likewise, pooled AB serum at these concentrations has no effect (data not shown). In the presence of 5% serum but no IA-2ic-HA307–319, there is no T-cell activation. Data represent one of four experiments using four different cell donors. D: Pooled data from a total of four donors (including the one used in A) for plasmacytoid dendritic cell enhancement of IA-2ic-HA307–319 (▪) presentation to JNZ-1 clone cells (*P < 0.05, **P < 0.01, and ***P < 0.001 vs. presence of antigen alone; □). The additional sera contained 3,875.1, 3,263.1, and 3,007.8 WHO units of IA-2 autoantibodies. Bars represent means ± SE from quadruplicate wells of individual experiments. E: IA-2+ serum–enhanced IA-2ic-HA307–319 presentation is dependent on the serum IgG fraction. Serum has been adsorbed using Protein A matrix. Serum IgG level before adsorption, 6.54 g/l; after adsorption, 0.22 g/l. Serum was used at 5% concentration in these experiments. Serum IA-2 autoantibody level before adsorption, 2,152 WHO units; after adsorption, IA-2 autoantibodies were not detectable. *Significant reduction in IFN-γ production by clone JNZ-1 in the presence of adsorbed compared with nonadsorbed serum (P < 0.05).Comment in
-
Role of plasmacytoid dendritic cells in type 1 diabetes: friend or foe?Diabetes. 2009 Jan;58(1):12-3. doi: 10.2337/db08-1341. Diabetes. 2009. PMID: 19114722 Free PMC article. No abstract available.
References
-
- Tree TI, Peakman M: Autoreactive T cells in human type 1 diabetes. Endocrinol Metab Clin North Am 33: 113–133, ix–x, 2004 - PubMed
-
- Atkinson MA, Eisenbarth GS: Type 1 diabetes: new perspectives on disease pathogenesis and treatment. Lancet 358: 221–229, 2001 - PubMed
-
- Roep BO: The role of T-cells in the pathogenesis of type 1 diabetes: from cause to cure. Diabetologia 46: 305–321, 2003 - PubMed
-
- Steinman RM, Hemmi H: Dendritic cells: translating innate to adaptive immunity. Curr Top Microbiol Immunol 311: 17–58, 2006 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
