

Endometriosis and Chronic Pelvic Pain: Unraveling the Mystery Behind this Complex Condition
- PMID: 18837717
- PMCID: PMC3096669
- DOI: 10.1111/j.1751-486X.2008.00362.x
Endometriosis and Chronic Pelvic Pain: Unraveling the Mystery Behind this Complex Condition
Abstract
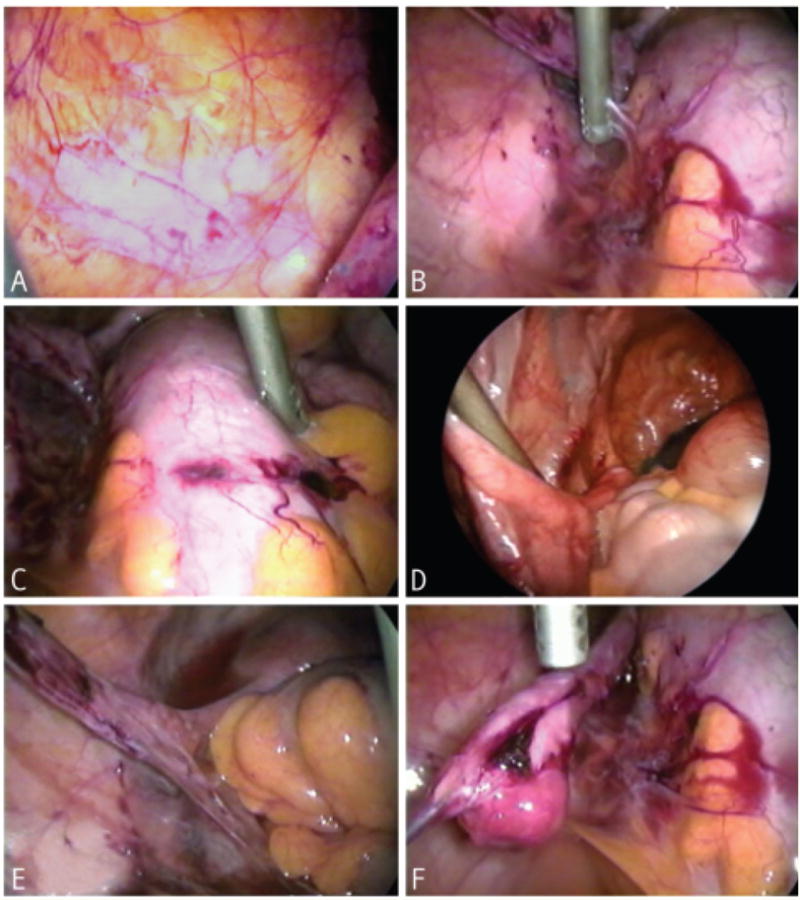
Nurses often encounter patients with chronic pelvic pain associated with endometriosis, which is a puzzling and problematic gynecologic condition that has continued to plague women and baffle doctors and researchers worldwide since it was first identified by Dr. J. Sampson in the 1920s (Sampson, 1940). Endometriosis is defined as the growth, adhesion and progression of endometrial glands and stroma outside of the uterine cavity, with cellular activity evident in lesions, nodules, cysts or endometriomas (Audebert et al., 1992). Although it typically appears benign on histopathology, endometriosis has been likened to a malignant tumor since the lesions grow, infiltrate and adhere to adjacent tissues and interfere with physiologic processes (Kitawaki et al., 2002; Noble, Simpson, Johns, & Bulun, 1996). Ectopic endometriotic growths respond to cyclic changes of estrogen and proliferate and shed in a manner similar to eutopic endometrium. This cyclic ectopic activity results in internal bleeding, formation of scar tissue, inflammation and sometimes debilitating chronic pain (Kitawaki et al.).
Figures
References
-
- Ailawadi RK, Jobanpufra S, Kataria M, Gurates B, Bulun SE. Treatment of endometriosis and chronic pelvic pain with Letrozole and norethindrone acetate: A pilot study. Fertility and Sterility. 2004;81(2):290–296. - PubMed
-
- Alford D. Nursing care of the patient with endometriosis. Nursing Clinics of North America. 1968;3(2):217–227. - PubMed
-
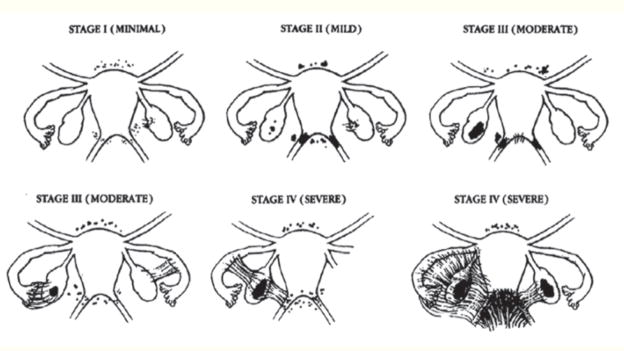
- American Society for Reproductive Medicine. Revised American society for reproductive medicine classification of endometriosis: 1996. Fertility and Sterility. 1996;67(5):817–821. - PubMed
-
- American Society for Reproductive Medicine. Endometriosis and infertility. Fertility and Sterility. 2006;86(4):156–160. - PubMed
-
- Attar E, Bulun SE. Aromatase inhibitors: The next generation of therapeutics for endometriosis? Fertility and Sterility. 2006;85(5):1307–1318. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
