

Tumor growth rates derived from data for patients in a clinical trial correlate strongly with patient survival: a novel strategy for evaluation of clinical trial data
- PMID: 18838440
- PMCID: PMC3313464
- DOI: 10.1634/theoncologist.2008-0075
Tumor growth rates derived from data for patients in a clinical trial correlate strongly with patient survival: a novel strategy for evaluation of clinical trial data
Abstract
Purpose: The slow progress in developing new cancer therapies can be attributed in part to the long time spent in clinical development. To hasten development, new paradigms especially applicable to patients with metastatic disease are needed.
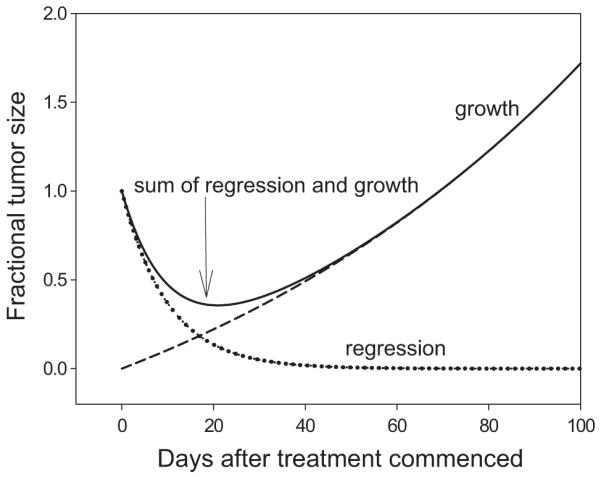
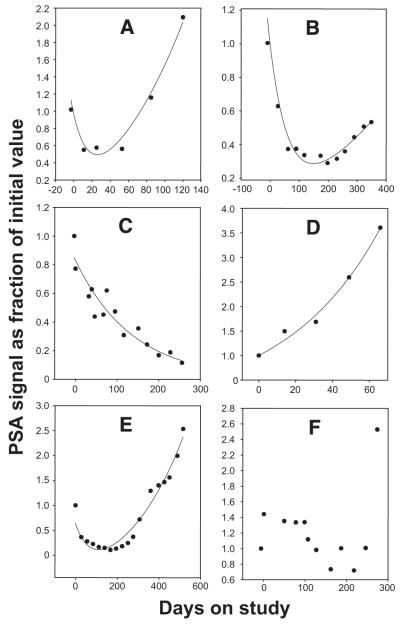
Patients and methods: We present a new method to predict survival using tumor measurement data gathered while a patient with cancer is receiving therapy in a clinical trial. We developed a two-phase equation to estimate the concomitant rates of tumor regression (regression rate constant d) and tumor growth (growth rate constant g).
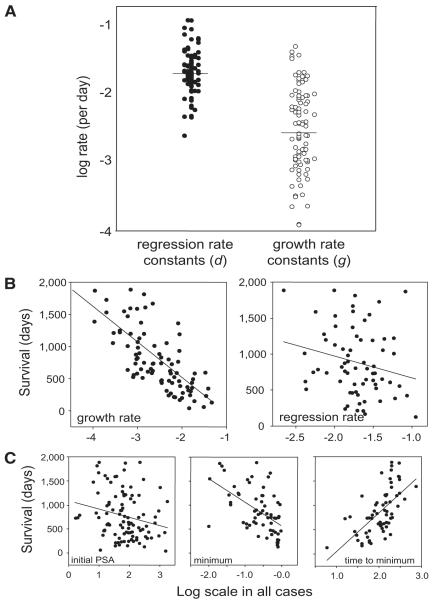
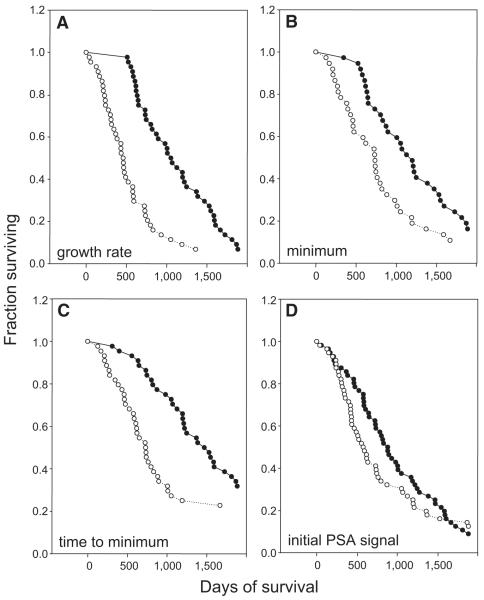
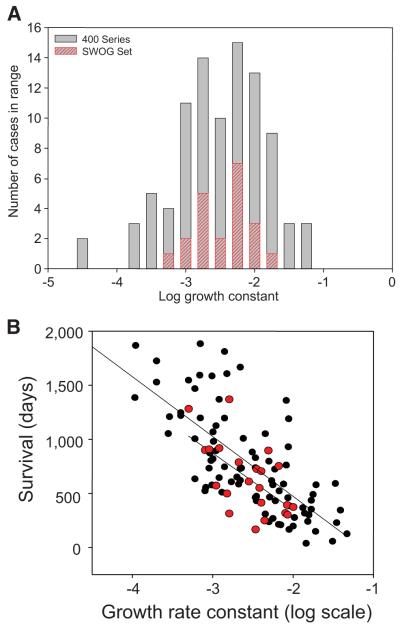
Results: We evaluated the model against serial levels of prostate-specific antigen (PSA) in 112 patients undergoing treatment for prostate cancer. Survival was strongly correlated with the log of the growth rate constant, log(g) (Pearson r = -0.72) but not with the log of the regression rate constants, log(d) (r = -0.218). Values of log(g) exhibited a bimodal distribution. Patients with log(g) values above the median had a mortality hazard of 5.14 (95% confidence interval, 3.10-8.52) when compared with those with log(g) values below the median. Mathematically, the minimum PSA value (nadir) and the time to this minimum are determined by the kinetic parameters d and g, and can be viewed as surrogates.
Conclusions: This mathematical model has applications to many tumor types and may aid in evaluating patient outcomes. Modeling tumor progression using data gathered while patients are on study, may help evaluate the ability of therapies to prolong survival and assist in drug development.
Figures
Comment in
-
Commentary: tumor growth, patient survival, and the search for the optimal phase II efficacy endpoint.Oncologist. 2008 Oct;13(10):1043-5. doi: 10.1634/theoncologist.2008-0180. Epub 2008 Oct 1. Oncologist. 2008. PMID: 18832191 No abstract available.
References
-
- Adams J. The development of proteasome inhibitors as anticancer drugs. Cancer Cell. 2004;5:417–421. - PubMed
-
- Sharifi N, Gulley JL, Dahut WL. Androgen deprivation therapy for prostate cancer. JAMA. 2005;294:238–244. - PubMed
-
- Petrylak D. Therapeutic options in androgen-independent prostate cancer: Building on docetaxel. BJU Int. 2005;96(suppl 2):41–46. - PubMed
-
- Pienta KJ, Bradley D. Mechanisms underlying the development of androgen-independent prostate cancer. Clin Cancer Res. 2006;12:1665–1671. - PubMed
-
- Silvestris N, Leone B, Numico G, et al. Present status and perspectives in the treatment of hormone-refractory prostate cancer. Oncology. 2005;69:273–282. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
