

Evaluating test strategies for colorectal cancer screening: a decision analysis for the U.S. Preventive Services Task Force
- PMID: 18838717
- PMCID: PMC2731975
- DOI: 10.7326/0003-4819-149-9-200811040-00244
Evaluating test strategies for colorectal cancer screening: a decision analysis for the U.S. Preventive Services Task Force
Abstract
Background: The U.S. Preventive Services Task Force requested a decision analysis to inform their update of recommendations for colorectal cancer screening.
Objective: To assess life-years gained and colonoscopy requirements for colorectal cancer screening strategies and identify a set of recommendable screening strategies.
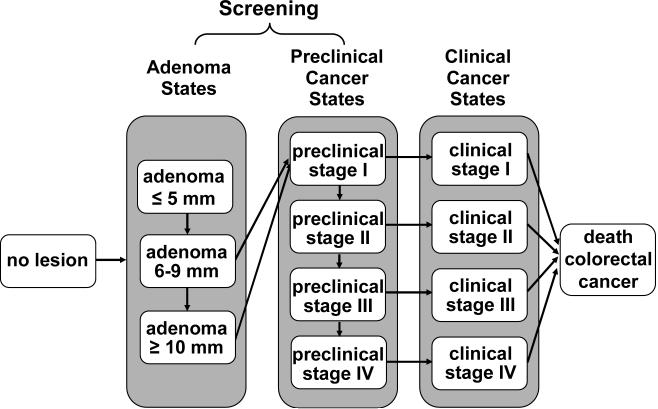
Design: Decision analysis using 2 colorectal cancer microsimulation models from the Cancer Intervention and Surveillance Modeling Network.
Data sources: Derived from the literature.
Target population: U.S. average-risk 40-year-old population.
Perspective: Societal.
Time horizon: Lifetime.
Interventions: Fecal occult blood tests (FOBTs), flexible sigmoidoscopy, or colonoscopy screening beginning at age 40, 50, or 60 years and stopping at age 75 or 85 years, with screening intervals of 1, 2, or 3 years for FOBT and 5, 10, or 20 years for sigmoidoscopy and colonoscopy.
Outcome measures: Number of life-years gained compared with no screening and number of colonoscopies and noncolonoscopy tests required.
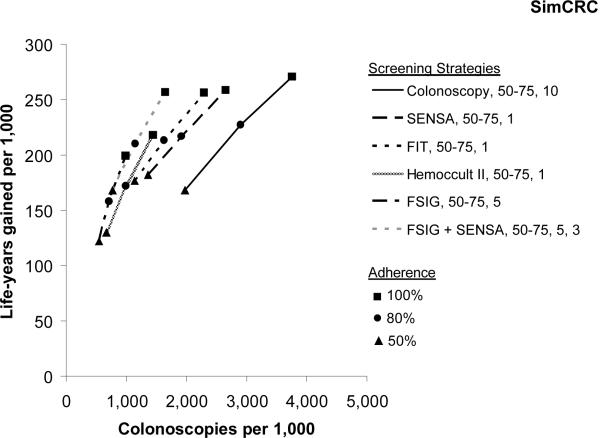
Results of base-case analysis: Beginning screening at age 50 years was consistently better than at age 60. Decreasing the stop age from 85 to 75 years decreased life-years gained by 1% to 4%, whereas colonoscopy use decreased by 4% to 15%. Assuming equally high adherence, 4 strategies provided similar life-years gained: colonoscopy every 10 years, annual Hemoccult SENSA (Beckman Coulter, Fullerton, California) testing or fecal immunochemical testing, and sigmoidoscopy every 5 years with midinterval Hemoccult SENSA testing. Annual Hemoccult II and flexible sigmoidoscopy every 5 years alone were less effective.
Results of sensitivity analysis: The results were most sensitive to beginning screening at age 40 years.
Limitation: The stop age for screening was based only on chronologic age.
Conclusion: The findings support colorectal cancer screening with the following: colonoscopy every 10 years, annual screening with a sensitive FOBT, or flexible sigmoidoscopy every 5 years with a midinterval sensitive FOBT from age 50 to 75 years.
Figures




Comment in
-
Screening guidelines for colorectal cancer: a twice-told tale.Ann Intern Med. 2008 Nov 4;149(9):680-2. doi: 10.7326/0003-4819-149-9-200811040-00247. Epub 2008 Oct 7. Ann Intern Med. 2008. PMID: 18840787 No abstract available.
-
Will test-specific adherence predict the best colorectal cancer screening strategy?Ann Intern Med. 2009 Mar 3;150(5):359; author reply 359-60. doi: 10.7326/0003-4819-150-5-200903030-00019. Ann Intern Med. 2009. PMID: 19258565 No abstract available.
Summary for patients in
-
Summaries for patients. Screening for colorectal cancer: U.S. Preventive Services Task Force recommendation.Ann Intern Med. 2008 Nov 4;149(9):I-44. doi: 10.7326/0003-4819-149-9-200811040-00246. Epub 2008 Oct 6. Ann Intern Med. 2008. PMID: 18838719 No abstract available.
References
-
- Jemal A, Clegg LX, Ward E, Ries LA, Wu X, Jamison PM, et al. Annual report to the nation on the status of cancer, 1975-2001, with a special feature regarding survival. Cancer. 2004;101:3–27. [PMID: 15221985] - PubMed
-
- American Cancer Society . Cancer Facts and Figures 2008. Accessed at www.cancer.org/downloads/STT/2008CAFFfinalsecured.pdf on September 15, 2008.
-
- Mandel JS, Bond JH, Church TR, Snover DC, Bradley GM, Schuman LM, et al. Reducing mortality from colorectal cancer by screening for fecal occult blood. Minnesota Colon Cancer Control Study. N Engl J Med. 1993;328:1365–71. [PMID: 8474513] - PubMed
-
- Hardcastle JD, Chamberlain JO, Robinson MH, Moss SM, Amar SS, Balfour TW, et al. Randomised controlled trial of faecal-occult-blood screening for colorectal cancer. Lancet. 1996;348:1472–7. [PMID: 8942775] - PubMed
-
- Kronborg O, Fenger C, Olsen J, Jørgensen OD, Søndergaard O. Randomised study of screening for colorectal cancer with faecal-occult-blood test. Lancet. 1996;348:1467–71. [PMID: 8942774] - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials