

Aortic dissection in Turner syndrome
- PMID: 18839441
- PMCID: PMC2692924
- DOI: 10.1097/hco.0b013e3283129b89
Aortic dissection in Turner syndrome
Abstract
Purpose of review: Turner syndrome is a relatively common disorder of female development with cardinal features of short stature and congenital cardiovascular defects (CHD). Turner syndrome is the most common established cause of aortic dissection in young women, but has received little attention outside pediatric literature. This review focuses on emerging knowledge of the characteristics of aortic disease in Turner syndrome in comparison with Marfan-like syndromes and isolated aortic valve disease.
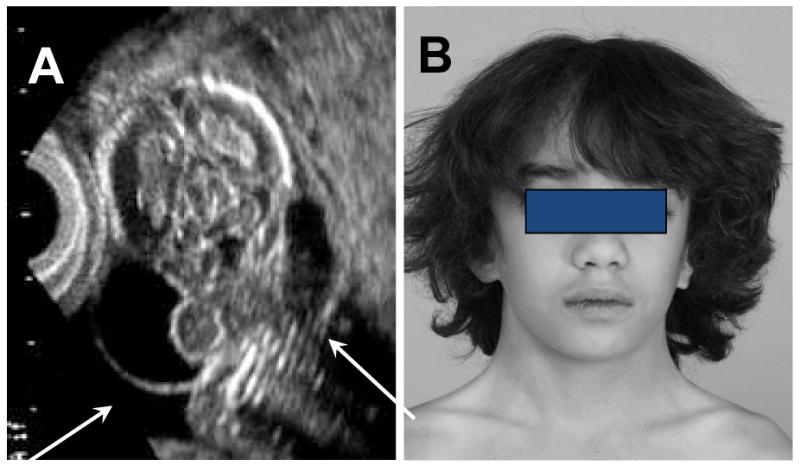
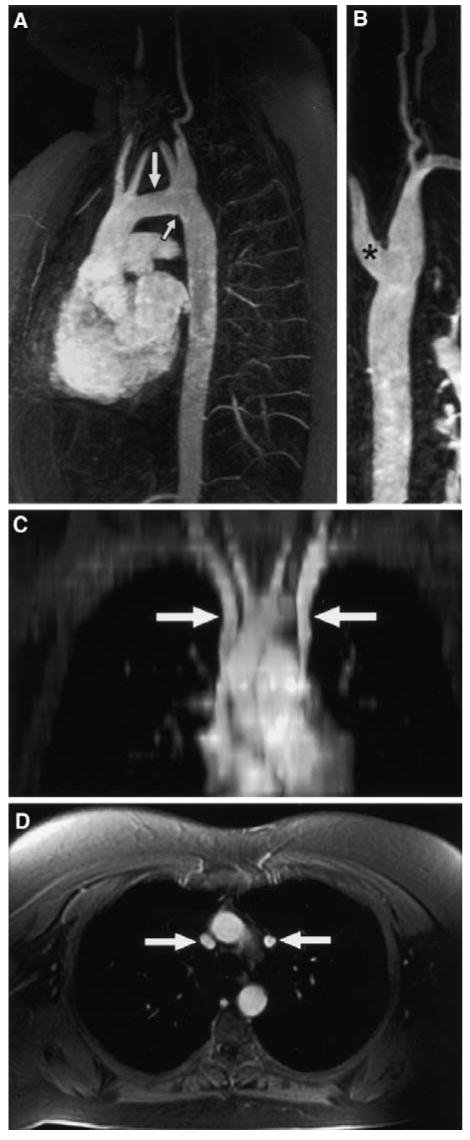
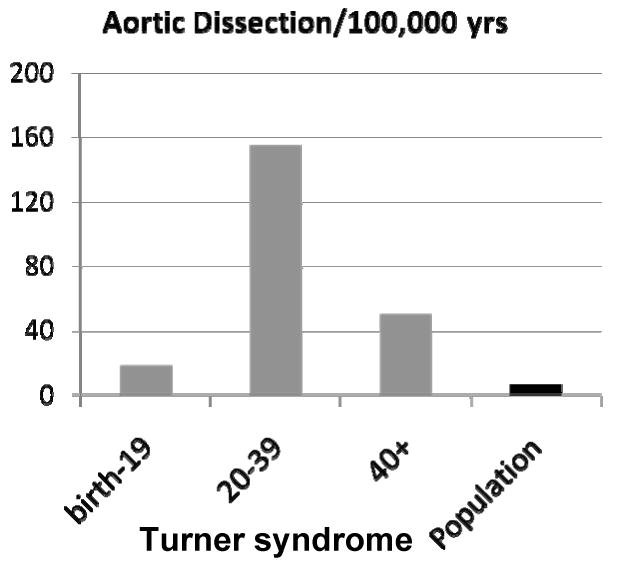
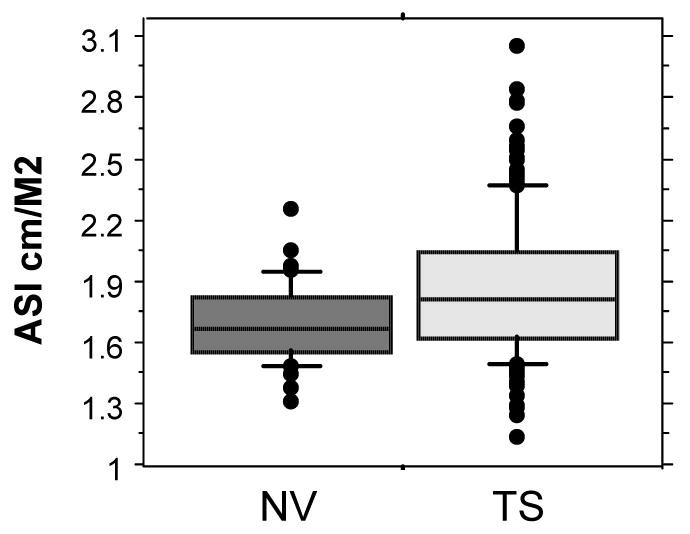
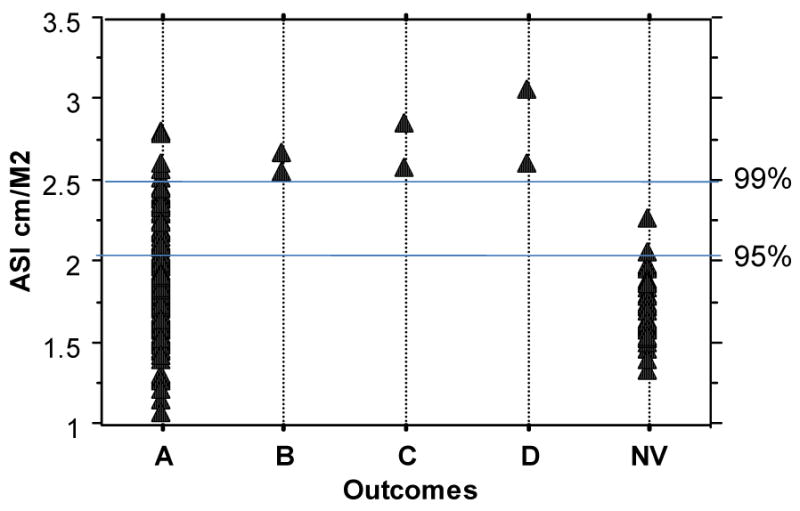
Recent findings: The incidence of aortic dissection is significantly increased in individuals with Turner syndrome at all ages, highest during young adult years and in pregnancy. Pediatric patients with dissection have known congenital cardiovascular defects (CHD), but adults often have aortic valve and arch abnormalities detected only by screening cardiac magnetic resonance. Thoracic aortic dilation in Turner syndrome must be evaluated in relation to body surface area. Dilation is most prominent at the ascending aorta, similar to the pattern seen in nonsyndromic bicuspid aortic valve, is equally prevalent (20-30%) in children and adults, and does not seem to be rapidly progressive. Cardiovascular anomalies and risk for aortic dissection in Turner syndrome are strongly linked to a history of fetal lymphedema, evidenced by the presence of neck webbing and shield chest.
Summary: Risk for acute aortic dissection is increased by more than 100-fold in young and middle-aged women with Turner syndrome. Monitoring frequency and treatment modalities are decided on an individual basis until more information on outcomes becomes available.
Conflict of interest statement
The author has no disclosures.
Figures
References
-
- Stochholm K, Juul S, Juel K, et al. Prevalence, Incidence, Diagnostic Delay, and Mortality in Turner Syndrome. J Clin Endocrinol Metab. 2006;91:3897–3902. - PubMed
-
- Hook EB, Warburton D. The distribution of chromosomal genotypes associated with Turner's syndrome: livebirth prevalence rates and evidence for diminished fetal mortality and severity in genotypes associated with structural X abnormalities or mosaicism. Hum Genet. 1983;64:24–27. - PubMed
-
- Surerus E, Huggon IC, Allan LD. Turner's syndrome in fetal life. Ultrasound Obstet Gynecol. 2003;22:264–267. - PubMed
-
- Ross J, Roeltgen D, Zinn A. Cognition and the sex chromosomes: studies in Turner syndrome. Horm Res. 2006;65:47–56. - PubMed
-
- *Bondy CA. Care of Girls and Women with Turner Syndrome: A Guideline of the Turner Syndrome Study Group. J Clin Endocrinol Metab. 2007;92:10–25. - PubMed
-
Consensus recommendations for multidisciplinary care.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
