

Bone graft harvest using a new intramedullary system
- PMID: 18841433
- PMCID: PMC2628246
- DOI: 10.1007/s11999-008-0538-3
Bone graft harvest using a new intramedullary system
Abstract
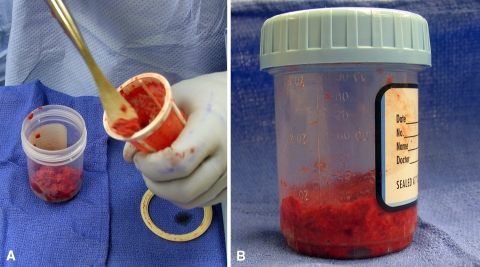
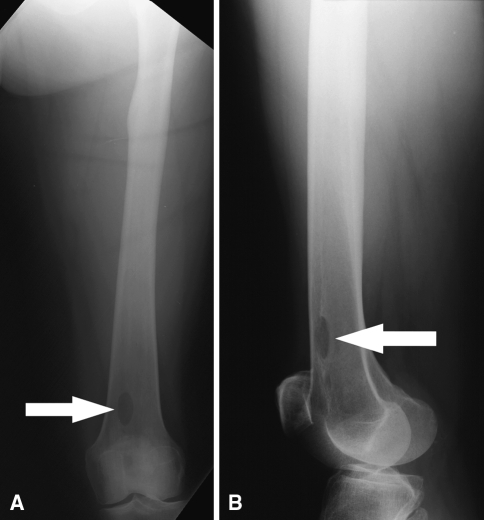
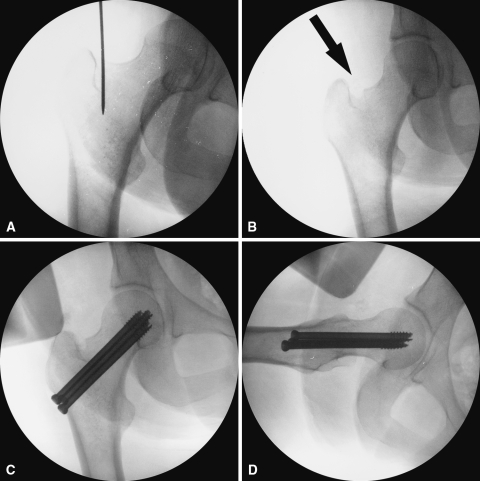
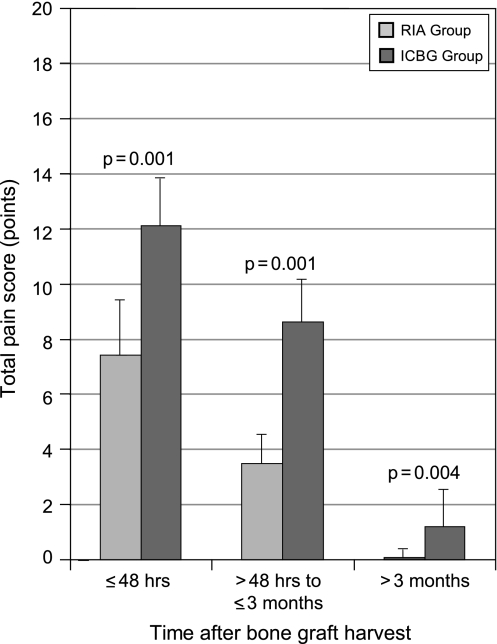
Obtaining autogenous bone graft from the iliac crest can entail substantial morbidity. Alternatively, bone graft can be harvested from long bones using an intramedullary (IM) harvesting system. We measured bone graft volume obtained from the IM canals of the femur and tibia and documented the complications of the harvesting technique. Donor site pain and the union rate were compared between the IM and the traditional iliac crest bone graft (ICBG) harvest. Forty-one patients (23 male, 18 female) with an average age of 44.9 years (range, 15-78 years) had graft harvested from long bones using an IM harvest system (femoral donor site, 37 patients; tibial donor site, four patients). Forty patients (23 male, 17 female; average age, 46.4 years; range, 15-77 years) underwent anterior ICBG harvest. We administered patient surveys to both groups to determine pain intensity and frequency. IM group reported lower pain scores than the ICBG group during all postoperative periods. Mean graft volume for the IM harvest group was 40.3 mL (range, 25-75 mL) (graft volume was not obtained for the ICBG group). Using an intramedullary system to harvest autogenous bone graft from the long bones is safe provided a meticulous technique is used.
Level of evidence: Level III, retrospective comparative study. See the Guidelines for Authors for a complete description of levels of evidence.
Figures



Comment in
-
Re: Bone graft harvest using a new intramedullary system.Clin Orthop Relat Res. 2009 Oct;467(10):2749. doi: 10.1007/s11999-009-0943-2. Epub 2009 Jun 30. Clin Orthop Relat Res. 2009. PMID: 19565306 Free PMC article. No abstract available.
References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1302/0301-620X.84B5.12571', 'is_inner': False, 'url': 'https://doi.org/10.1302/0301-620x.84b5.12571'}, {'type': 'PubMed', 'value': '12004011', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/12004011/'}]}
- Ahlmann E, Patzakis M, Roidis N, Shepherd L, Holtman P. Comparison of anterior and posterior iliac crest bone grafts in terms of harvest-site morbidity and functional outcomes. J Bone Joint Surg Am. 2002;84:716–720. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '16958471', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/16958471/'}]}
- Bedi A, Karunakar MA. Physiologic effects of intramedullary reaming. Instr Course Lect. 2006;55:359–366. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '4192328', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/4192328/'}]}
- Danckwardt-Lillieström G. Reaming of the medullary cavity and its effect on diaphyseal bone. A fluorochromic, microangiographic and histologic study on the rabbit tibia and dog femur. Acta Orthop Scand Suppl. 1969;128:1–153. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '11421578', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/11421578/'}]}
- Ebraheim NA, Elgafy H, Xu R. Bone-graft harvesting from iliac and fibular donor sites: techniques and complications. J Am Acad Ortho Surg. 2001;9:210–218. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '17695343', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/17695343/'}]}
- Faul F, Erdfelder E, Lang A-G, Buchner A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39:175–191. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
