

A tissue biomarker panel predicting systemic progression after PSA recurrence post-definitive prostate cancer therapy
- PMID: 18846227
- PMCID: PMC2565588
- DOI: 10.1371/journal.pone.0002318
A tissue biomarker panel predicting systemic progression after PSA recurrence post-definitive prostate cancer therapy
Abstract
Background: Many men develop a rising PSA after initial therapy for prostate cancer. While some of these men will develop a local or metastatic recurrence that warrants further therapy, others will have no evidence of disease progression. We hypothesized that an expression biomarker panel can predict which men with a rising PSA would benefit from further therapy.
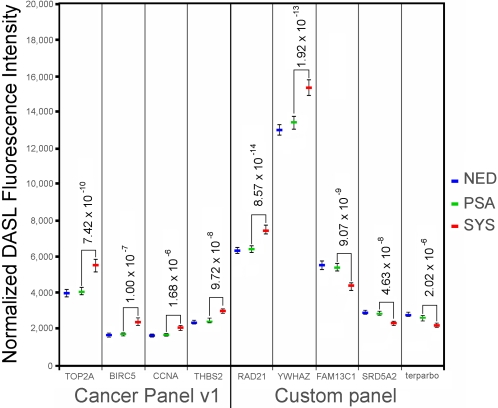
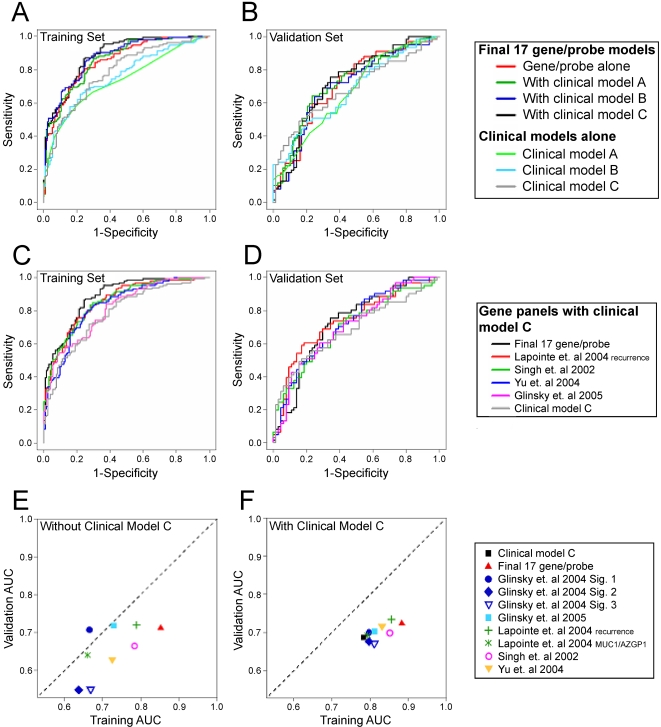
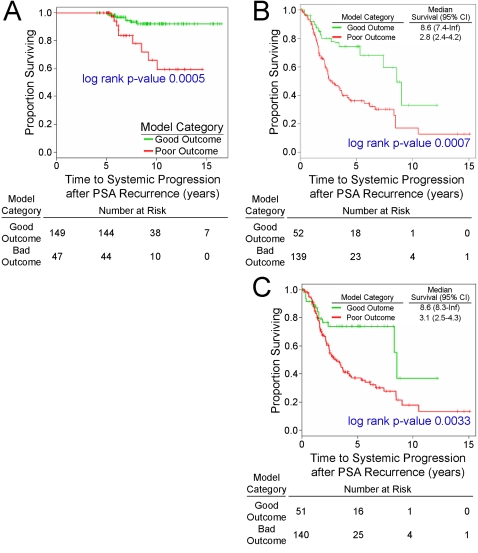
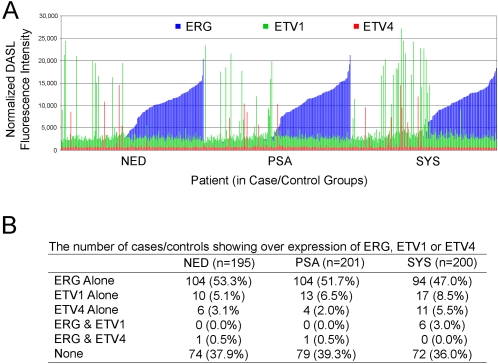
Methodology/principal findings: A case-control design was used to test the association of gene expression with outcome. Systemic (SYS) progression cases were men post-prostatectomy who developed systemic progression within 5 years after PSA recurrence. PSA progression controls were matched men post-prostatectomy with PSA recurrence but no evidence of clinical progression within 5 years. Using expression arrays optimized for paraffin-embedded tissue RNA, 1021 cancer-related genes were evaluated-including 570 genes implicated in prostate cancer progression. Genes from 8 previously reported marker panels were included. A systemic progression model containing 17 genes was developed. This model generated an AUC of 0.88 (95% CI: 0.84-0.92). Similar AUCs were generated using 3 previously reported panels. In secondary analyses, the model predicted the endpoints of prostate cancer death (in SYS cases) and systemic progression beyond 5 years (in PSA controls) with hazard ratios 2.5 and 4.7, respectively (log-rank p-values of 0.0007 and 0.0005). Genes mapped to 8q24 were significantly enriched in the model.
Conclusions/significance: Specific gene expression patterns are significantly associated with systemic progression after PSA recurrence. The measurement of gene expression pattern may be useful for determining which men may benefit from additional therapy after PSA recurrence.
Conflict of interest statement
Figures
References
-
- Jemal A, Murray T, Ward E, Samuels A, Tiwari RC, et al. Cancer statistics. CA Cancer J Clin. 2005;55:10–30. - PubMed
-
- D'Amico AV, Moul J, Carroll PR, Sun L, Lubeck D, et al. Cancer-specific mortality after surgery or radiation for patients with clinically localized prostate cancer managed during the prostate-specific antigen era. J Clin Oncol. 2003;21:2163–72. - PubMed
-
- Amling CL, Blute ML, Bergstralh EJ, Seay TM, Slezak J, et al. Long-term hazard of progression after radical prostatectomy for clinically localized prostate cancer: continued risk of biochemical failure after 5 years. J Urol. 2000;164:101–5. - PubMed
-
- Shipley WU, Thames HD, Sandler HM, Hanks GE, Zietman AL, et al. Radiation therapy for clinically localized prostate cancer: a multi-institutional pooled analysis. JAMA. 1999;281:1598–604. - PubMed
-
- Patel DA, Presti JC, Jr, McNeal JE, Gill H, Brooks JD, et al. Preoperative PSA velocity is an independent prognostic factor for relapse after radical prostatectomy. J Clin Oncol. 2005;23:6157–62. - PubMed
MeSH terms
Substances
Associated data
- Actions
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
