

Review
doi: 10.1016/j.jpeds.2008.05.062.
Dyslipidemia in youth with diabetes: to treat or not to treat?
Affiliations
- PMID: 18847618
- PMCID: PMC2585025
- DOI: 10.1016/j.jpeds.2008.05.062
Item in Clipboard
Review
Dyslipidemia in youth with diabetes: to treat or not to treat?
J Pediatr.
2008 Oct.
No abstract available
Figures
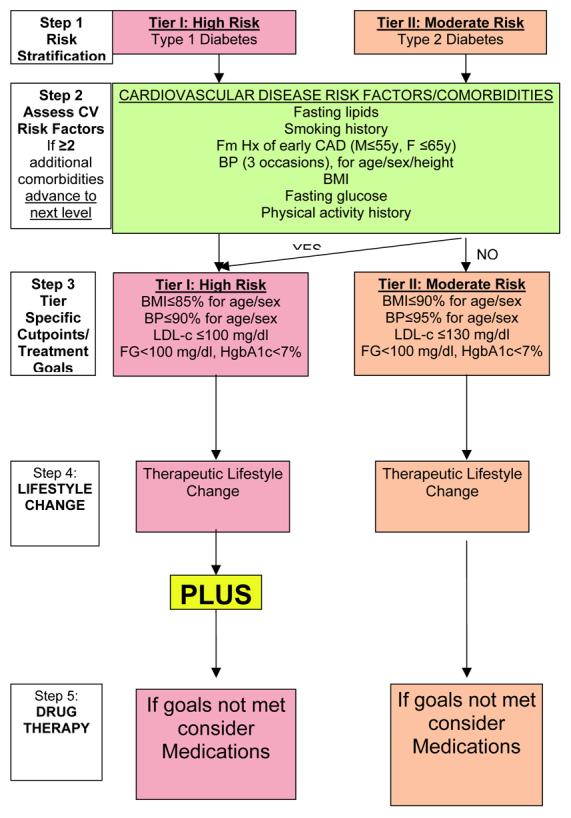
[adapted from Kavey(29)]
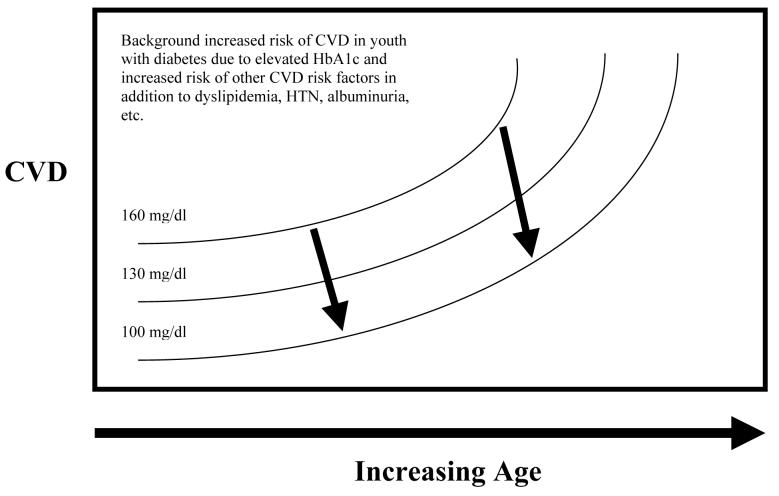
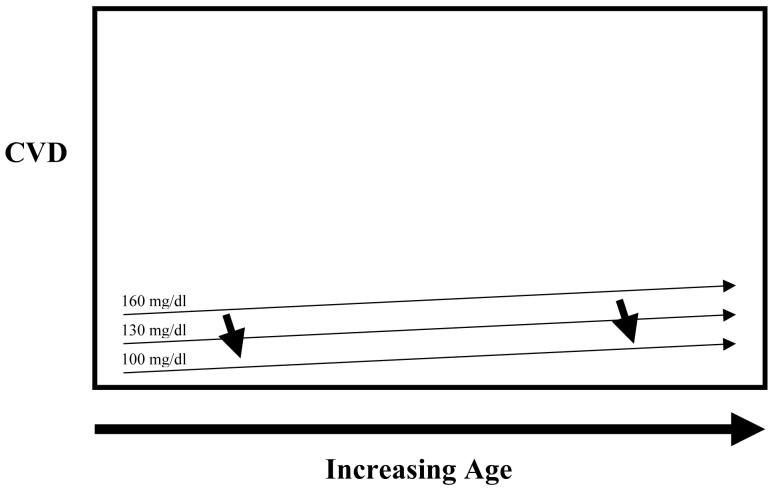
Youth with diabetes are at increased risk of future cardiovascular disease. The question remains as to the timing of pharmacologic intervention. Numerous factors influence this decision including background risk of CVD for youth with diabetes, safety of pharmacologic agents, degree of long-term benefit to be gained from intervention, etc. Currently, data are insufficient to determine the degree of benefit to be obtained from early intervention on CVD risk factors in youth with diabetes in reducing this cumulative area under the curve of CVD risk factors. Figure 2A represents possible long-term risk reduction assuming high background CVD risk and benefit from LDL-c lowering, and Figure 2B represents lower background CVD risk and less benefit from LDL-c lowering.
Youth with diabetes are at increased risk of future cardiovascular disease. The question remains as to the timing of pharmacologic intervention. Numerous factors influence this decision including background risk of CVD for youth with diabetes, safety of pharmacologic agents, degree of long-term benefit to be gained from intervention, etc. Currently, data are insufficient to determine the degree of benefit to be obtained from early intervention on CVD risk factors in youth with diabetes in reducing this cumulative area under the curve of CVD risk factors. Figure 2A represents possible long-term risk reduction assuming high background CVD risk and benefit from LDL-c lowering, and Figure 2B represents lower background CVD risk and less benefit from LDL-c lowering.
Comment in
-
Relation between low-density lipoprotein particle size and insulin and diabetes mellitus.J Pediatr. 2009 Oct;155(4):600. doi: 10.1016/j.jpeds.2009.05.036. J Pediatr. 2009. PMID: 19773013 No abstract available.
References
-
- Liese AD, D'Agostino RB, Jr., Hamman RF, Kilgo PD, Lawrence JM, Liu LL, et al. The burden of diabetes mellitus among US youth: prevalence estimates from the SEARCH for Diabetes in Youth Study. Peds. 2006;118:1510–1518. - PubMed
-
- EURODIAB ACE Study Group Variation and trends in incidence of childhood diabetes in Europe. Lancet. 2000;355:873–876. - PubMed
-
- Pinhas-Hamiel O, Zeitler P. The global spread of type 2 diabetes mellitus in children and adolescents. J Pediatr. 2005;146:693–700. - PubMed
-
- Vehik K, Hamman RF, Lezotte D, Norris JM, Klingensmith G, Bloch C, et al. Increasing incidence of type 1 diabetes in 0- to 17-year-old Colorado youth. Diab Care. 2007;30:503–509. - PubMed
-
- Pavkov ME, Bennett PH, Knowler WC, Krakoff J, Sievers ML, Nelson RG. Effect of youth-onset type 2 diabetes mellitus on incidence of end-stage renal disease and mortality in young and middle-aged Pima Indians. JAMA. 2006;296:421–426. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
