

Cost effectiveness of alternative surveillance strategies for hepatocellular carcinoma in patients with cirrhosis
- PMID: 18848905
- PMCID: PMC4340842
- DOI: 10.1016/j.cgh.2008.08.005
Cost effectiveness of alternative surveillance strategies for hepatocellular carcinoma in patients with cirrhosis
Abstract
Background & aims: The increasing incidence of hepatocellular carcinoma (HCC) in the United States has significant health and economic consequences. Ultrasound (US) surveillance is recommended for patients with cirrhosis because of their high risk of HCC and improving treatment outcomes for small tumors. We assessed the costs, clinical benefits, and cost effectiveness of US surveillance and alternative strategies for HCC in cirrhosis using a computer-based state transition model with parameters derived from available literature.
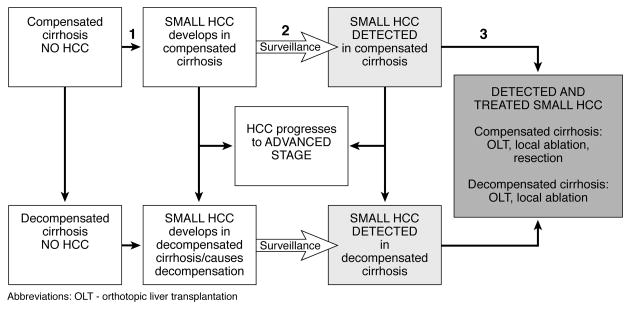
Methods: Our model compared a policy of no surveillance with 6 surveillance strategies in cirrhotic patients ages 50 years and older in the United States: (1) annual US, (2) semiannual US, (3) semiannual US with alpha-fetoprotein, (4) annual computed tomography (CT), (5) semiannual CT, and (6) annual magnetic resonance imaging. The number of screening tests needed to detect one small HCC, cost per treated HCC, lifetime costs, quality-adjusted life expectancy, and incremental cost-effectiveness ratios were calculated.
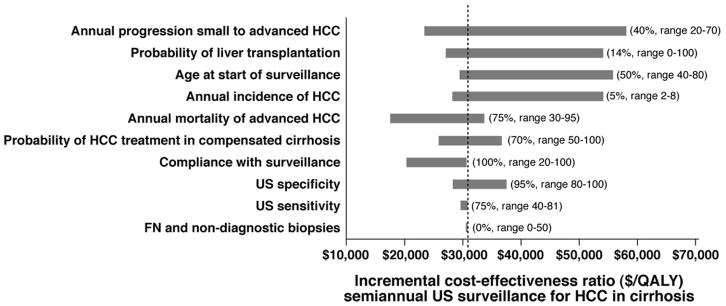
Results: Semiannual US surveillance for HCC in cirrhosis increased quality-adjusted life expectancy by 8.6 months on average, but extended it nearly 3.5 years in patients with small treated tumors. Semiannual US surveillance had an incremental cost-effectiveness ratio of $30,700 per quality-adjusted life year (QALY) gained, and was more cost effective than the alternative surveillance strategies using a threshold of $50,000 per QALY gained. The incremental cost-effectiveness ratios for the combined alpha-fetoprotein/US and annual CT strategies exceeded $50,000/QALY unless the sensitivity and specificity of US decreased to less than 65% and 60%, respectively.
Conclusions: Semiannual US surveillance for HCC in cirrhotic patients improves clinical outcomes at a reasonable cost.
Conflict of interest statement
Conflict of interest: No author has a conflict of interest to disclose.
Figures
Similar articles
-
Magnetic Resonance Imaging Is Cost-Effective for Hepatocellular Carcinoma Surveillance in High-Risk Patients With Cirrhosis.Hepatology. 2019 Apr;69(4):1599-1613. doi: 10.1002/hep.30330. Epub 2019 Feb 25. Hepatology. 2019. PMID: 30365164
-
Economic evaluation and budget impact analysis of the surveillance program for hepatocellular carcinoma in Thai chronic hepatitis B patients.Asian Pac J Cancer Prev. 2014;15(20):8993-9004. doi: 10.7314/apjcp.2014.15.20.8993. Asian Pac J Cancer Prev. 2014. PMID: 25374242
-
Cost-effectiveness of hepatocellular carcinoma surveillance in patients with hepatitis C virus-related cirrhosis.Clin Gastroenterol Hepatol. 2005 Jan;3(1):75-84. doi: 10.1016/s1542-3565(04)00443-4. Clin Gastroenterol Hepatol. 2005. PMID: 15645408
-
Surveillance for hepatocellular carcinoma.Semin Oncol. 2012 Aug;39(4):384-98. doi: 10.1053/j.seminoncol.2012.05.002. Semin Oncol. 2012. PMID: 22846857 Review.
-
Cost-effectiveness of liver cancer screening.Best Pract Res Clin Gastroenterol. 2013 Dec;27(6):961-72. doi: 10.1016/j.bpg.2013.08.021. Epub 2013 Oct 4. Best Pract Res Clin Gastroenterol. 2013. PMID: 24182614 Review.
Cited by
-
Redefining HCC Surveillance in India: A Call for Innovative and Inclusive Strategies.J Clin Exp Hepatol. 2024 Nov-Dec;14(6):101474. doi: 10.1016/j.jceh.2024.101474. Epub 2024 Jun 25. J Clin Exp Hepatol. 2024. PMID: 39108278 Review.
-
Current Trends and Characteristics of Hepatocellular Carcinoma in Patients with Autoimmune Liver Diseases.Cancers (Basel). 2021 Mar 1;13(5):1023. doi: 10.3390/cancers13051023. Cancers (Basel). 2021. PMID: 33804480 Free PMC article. Review.
-
Resection of NAFLD-Associated HCC: Patient Selection and Reported Outcomes.J Hepatocell Carcinoma. 2020 Jul 30;7:107-116. doi: 10.2147/JHC.S252506. eCollection 2020. J Hepatocell Carcinoma. 2020. PMID: 32802809 Free PMC article. Review.
-
Duration and cost-effectiveness of hepatocellular carcinoma surveillance in hepatitis C patients after viral eradication.J Hepatol. 2022 Jul;77(1):55-62. doi: 10.1016/j.jhep.2022.01.027. Epub 2022 Feb 12. J Hepatol. 2022. PMID: 35157959 Free PMC article.
-
Hepatocellular carcinoma surveillance: Eastern and Western perspectives.Ultrasonography. 2019 Jul;38(3):191-199. doi: 10.14366/usg.18043. Epub 2018 Oct 28. Ultrasonography. 2019. PMID: 30690962 Free PMC article.
References
-
- El-Serag HB. Hepatocellular carcinoma: recent trends in the United States. Gastroenterology. 2004;127(5 Suppl 1):S27–34. - PubMed
-
- El-Serag HB, Davila JA, Petersen NJ, et al. The continuing increase in the incidence of hepatocellular carcinoma in the United States: an update. Ann Intern Med. 2003;139(10):817–23. - PubMed
-
- Sandler RS, Everhart JE, Donowitz M, et al. The burden of selected digestive diseases in the United States. Gastroenterology. 2002;122(5):1500–11. - PubMed
-
- Chalasani N, Said A, Ness R, et al. Screening for hepatocellular carcinoma in patients with cirrhosis in the United States: results of a national survey. Am J Gastroenterol. 1999;94(8):2224–9. - PubMed
-
- Colombo M, Mannucci PM, Brettler DB, et al. Hepatocellular carcinoma in hemophilia. Am J Hematol. 1991;37(4):243–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
