

The usefulness of contrast during exercise echocardiography for the assessment of systolic pulmonary pressure
- PMID: 18851729
- PMCID: PMC2570360
- DOI: 10.1186/1476-7120-6-51
The usefulness of contrast during exercise echocardiography for the assessment of systolic pulmonary pressure
Abstract
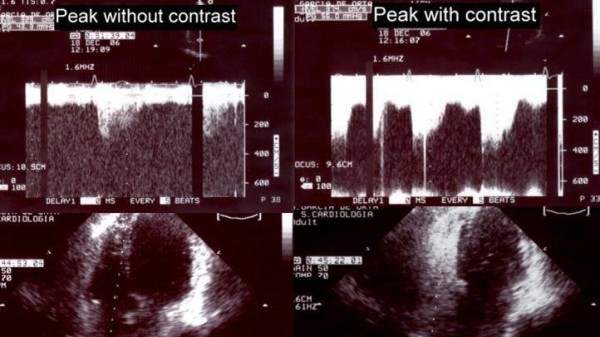
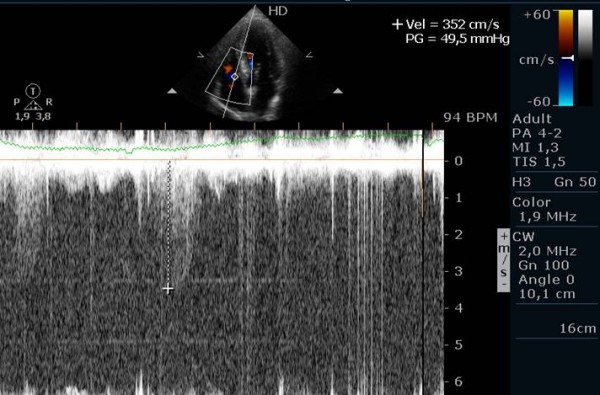
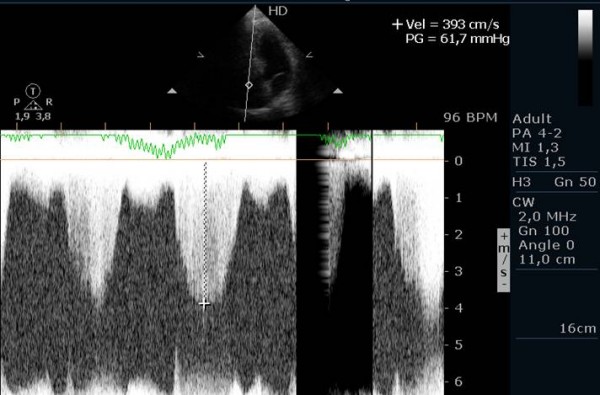
Background: The systolic pulmonary artery pressure (PAPs) can be accurately estimated, non-invasively, using continuous-wave Doppler (CWD) ultrasound measurement of the peak velocity of a tricuspid regurgitant (TR) jet. However, it is often difficult to obtain adequate tricuspid regurgitation signals for measurement of PAPs, what could lead to its underestimation. Therefore, utilization of air-blood-saline contrast has been implemented for the improvement of Doppler signal in several clinical contexts. It is now recommended in the evaluation of patients with pulmonary hypertension. Physical activity is severely restricted in patients with PAH, being exertional dypnea the most typical symptom. Exercise stress echo-Doppler imaging allows assessment of the response to exercise. It is an excellent screening test for patients with suspected PAH. Our purpose was to evaluate the value and accuracy of agitated saline with blood contrast echocardiography, in the improvement of the Doppler signal, to quantify PAPs during treadmill exercise-echocardiography.
Purpose: To evaluate the value of contrast echocardiography, using agitated saline with blood, in the improvement of the Doppler signal used to quantify the pulmonary artery systolic pressure during exercise.
Methods: From a total of 41 patients (pts), we studied 38 pts (93%), 35 women, aged 54 +/- 12 years-old. 27 with the diagnosis of systemic sclerosis, 10 with history of pulmonary embolism and one patient with a suspected idiopathic PAH, who were referred to the Unity of Heart Failure and Pulmonary Hypertension for screening of PAH. According to the Unity protocol, a transthoracic echocardiogram was made, in left decubitus (LD), with evaluation of right ventricle-right atria gradient (RV/RAg). A peripheral venous access was obtained, with a 3-way stopcock and the patients were placed in orthostatism (O), with a new evaluation of RV/RAg. Exercise echocardiography (EE) was begun, with evaluation of RV/RAg at peak exercise (P) and afterwards agitated saline (8 cc with 1 cc of air and 1 cc of blood) was injected, followed by a new evaluation of RV/RAg (PC) and then the interruption of the EE. Pulmonary Hypertension was diagnosed when RV/RAg at the end of the exercise was superior to 40 mmHg.
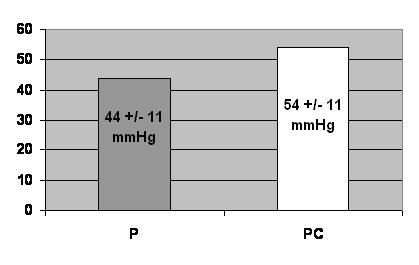
Results: The quality of Doppler signal was deteriorated in 5 pts, maintained in 6 pts and improved in 26 pts, with the use of contrast. In one patient, an interventricular septal defect was diagnosed. In 6 pts, a Doppler signal was only obtained with the use of contrast. In 15 pts, a RV/RAg superior to 40 mmHg was only obtained with the use of contrast. Of these, 9 have already been submitted to right heart cathetherism, that confirmed the diagnosis of pulmonary hypertension in 5 of them (56%). RV/RAg (P) was 44 +/- 11 mmHg and RV/RAg (PC) was 54 +/- 11 mmHg, p < 0,001.
Conclusion: 1. The method is applicable in a large number of patients. 2. RV/RA gradients obtained at peak exercise are higher with the use of contrast, and the clinical meaning of this difference should be evaluated in a larger number of pts submitted to right heart cathetherism. The high number of false positives should lead to a higher diagnostic threshold. 3. This method seems to have relevant clinical value in the diagnosis of pulmonary arterial hypertension.
Figures
Similar articles
-
Stress echocardiography in the evaluation of exercise physiology in patients with severe arterial pulmonary hypertension. New methodology.Rev Port Cardiol. 2005 Dec;24(12):1451-60. Rev Port Cardiol. 2005. PMID: 16566404 English, Portuguese.
-
Echocardiography during treadmill exercise testing for evaluation of pulmonary artery systolic pressure: advantages of the method.Rev Port Cardiol. 2008 Apr;27(4):453-61. Rev Port Cardiol. 2008. PMID: 18605064 English, Portuguese.
-
Noninvasive evaluation of systolic pressures of pulmonary artery and right ventricle using contrast-enhanced doppler echocardiography: comparative study using sonicated albumin or glucose solution.Pediatr Cardiol. 1996 May-Jun;17(3):175-80. doi: 10.1007/BF02505208. Pediatr Cardiol. 1996. PMID: 8662031
-
Doppler flow patterns in the evaluation of pulmonary hypertension.Rom J Intern Med. 2009;47(2):109-21. Rom J Intern Med. 2009. PMID: 20067161 Review.
-
Enhancing the accuracy of echocardiography in the diagnosis of pulmonary arterial hypertension: looking at the heart to learn about the lungs.Curr Opin Pulm Med. 2013 Sep;19(5):437-45. doi: 10.1097/MCP.0b013e3283645966. Curr Opin Pulm Med. 2013. PMID: 23884296 Review.
Cited by
-
Pulmonary Arterial Pressure Response During Exercise in COPD: A Correlation with C-Reactive Protein (hsCRP).Open Respir Med J. 2016 Jan 29;10:1-11. doi: 10.2174/1874306401610010001. eCollection 2016. Open Respir Med J. 2016. PMID: 27019674 Free PMC article.
-
Exploratory assessment of right ventricular structure and function during prolonged endurance cycling exercise.Echo Res Pract. 2023 Dec 20;10(1):22. doi: 10.1186/s44156-023-00035-8. Echo Res Pract. 2023. PMID: 38115147 Free PMC article.
-
Non-ischemic phenotypes of low-risk chest pain patients based on exercise stress echocardiography: a pilot study.Front Cardiovasc Med. 2025 Feb 19;12:1429449. doi: 10.3389/fcvm.2025.1429449. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 40046963 Free PMC article.
-
Noninvasive assessment of pulmonary vascular resistance and pressure in patients with congenital heart disease: a new method using M-mode echocardiography.J Echocardiogr. 2011 Dec;9(4):137-41. doi: 10.1007/s12574-011-0095-8. Epub 2011 Jun 11. J Echocardiogr. 2011. PMID: 27277290
-
Effect of oral nitrate supplementation on pulmonary hemodynamics during exercise and time trial performance in normoxia and hypoxia: a randomized controlled trial.Front Physiol. 2015 Oct 14;6:288. doi: 10.3389/fphys.2015.00288. eCollection 2015. Front Physiol. 2015. PMID: 26528189 Free PMC article.
References
-
- Yock PG, Popp RL. Noninvasive estimation of right ventricular systolic pressure by Doppler ultrasound in patients with tricuspid regurgitation. Circulation. 1984;70:657–62. - PubMed
-
- Berger M, Haimowitz A, Van Tosh A, Berdoff RL, Goldberg E. Quantitative assessment of pulmonary hypertension in patients with tricuspid regurgitation using continuous wave Doppler ultrasound. J Am Coll Cardiol. 1985;6:359–65. - PubMed
-
- Currie PJ, Seward JB, Chan KL, Fyfe DA, Hagler DJ, Mair DD, Reeder GS, Nishimura RA, Tajik AJ. Continuous wave Doppler determination of right ventricular pressure: a simultaneous Doppler-catheterization study in 127 patients. J Am Coll Cardiol. 1985;6:750–6. - PubMed
-
- Dubourg O, Delorme G, Jondeau G, Chikli F, Clavier H, Valtier B, Terdjman M, Beauchet A, Bourdarias JP. Simultaneous measurement of systolic pulmonary artery pressure by catheterization and contrast enhancement doppler echocardiography. Arch Mal Coeur Vaiss. 1993;86:1721–7. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
