

Transposition of the great arteries
- PMID: 18851735
- PMCID: PMC2577629
- DOI: 10.1186/1750-1172-3-27
Transposition of the great arteries
Abstract
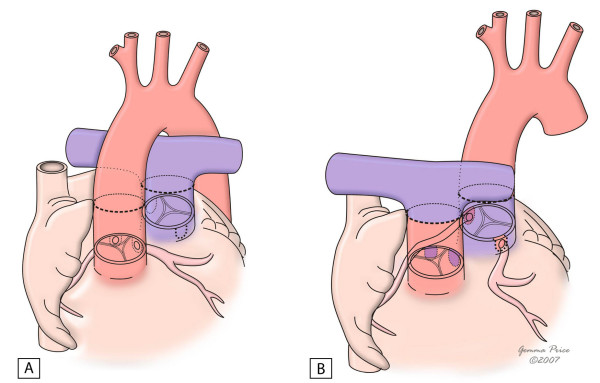
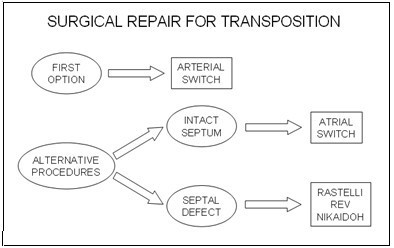
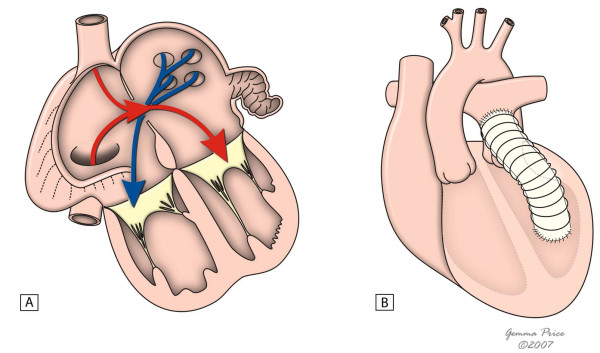
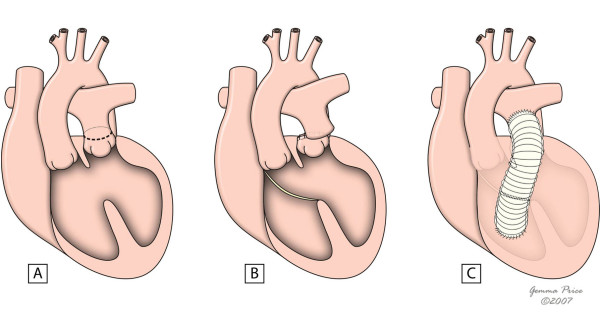
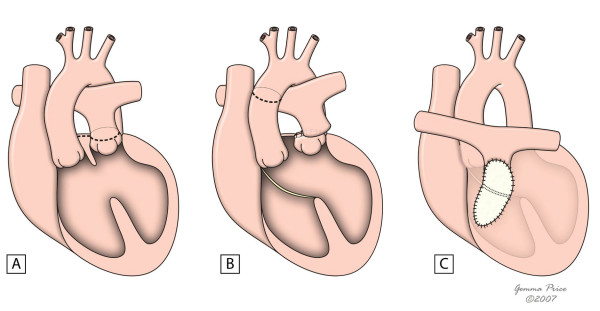
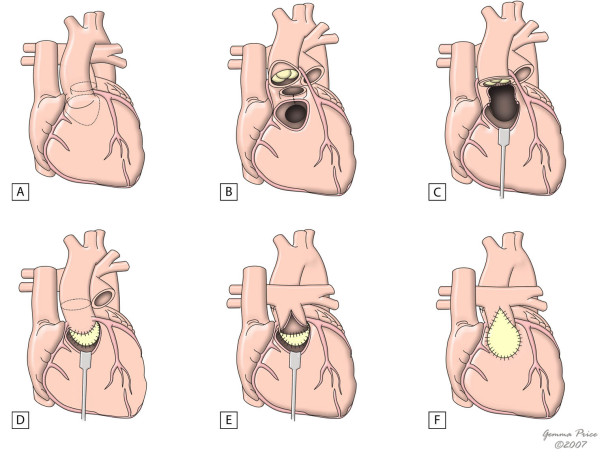
Transposition of the great arteries (TGA), also referred to as complete transposition, is a congenital cardiac malformation characterised by atrioventricular concordance and ventriculoarterial (VA) discordance. The incidence is estimated at 1 in 3,500-5,000 live births, with a male-to-female ratio 1.5 to 3.2:1. In 50% of cases, the VA discordance is an isolated finding. In 10% of cases, TGA is associated with noncardiac malformations. The association with other cardiac malformations such as ventricular septal defect (VSD) and left ventricular outflow tract obstruction is frequent and dictates timing and clinical presentation, which consists of cyanosis with or without congestive heart failure. The onset and severity depend on anatomical and functional variants that influence the degree of mixing between the two circulations. If no obstructive lesions are present and there is a large VSD, cyanosis may go undetected and only be perceived during episodes of crying or agitation. In these cases, signs of congestive heart failure prevail. The exact aetiology remains unknown. Some associated risk factors (gestational diabetes mellitus, maternal exposure to rodenticides and herbicides, maternal use of antiepileptic drugs) have been postulated. Mutations in growth differentiation factor-1 gene, the thyroid hormone receptor-associated protein-2 gene and the gene encoding the cryptic protein have been shown implicated in discordant VA connections, but they explain only a small minority of TGA cases.The diagnosis is confirmed by echocardiography, which also provides the morphological details required for future surgical management. Prenatal diagnosis by foetal echocardiography is possible and desirable, as it may improve the early neonatal management and reduce morbidity and mortality. Differential diagnosis includes other causes of central neonatal cyanosis. Palliative treatment with prostaglandin E1 and balloon atrial septostomy are usually required soon after birth. Surgical correction is performed at a later stage. Usually, the Jatene arterial switch operation is the procedure of choice. Whenever this operation is not feasible, adequate alternative surgical approach should be implemented. With the advent of newer and improved surgical techniques and post operative intensive care, the long-term survival is approximately 90% at 15 years of age. However, the exercise performance, cognitive function and quality of life may be impaired.
Figures
References
-
- Ho SY, Baker EJ, Rigby ML, Anderson RH. Color Atlas of Congenital Heart Disease – Morphologic and Clinical Correlations. Mosby-Wolfe, London; 1995.
-
- Houyel L, Van Praagh R, Lacour-Gayet F, Serraf A, Petit J, Bruniaux J, Planché C. Transposition of the great arteries [S, D, L]. Pathologic anatomy, diagnosis, and surgical management of a newly recognized complex. J Thorac Cardiovasc Surg. 1995;110:613–24. doi: 10.1016/S0022-5223(95)70092-7. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
