

Review
. 2008 Oct 4;8 Spec No A(Spec Iss A):S69-78.
doi: 10.1102/1470-7330.2008.9014.
Critical questions in the imaging of colorectal hepatic metastases
Affiliations
- PMID: 18852083
- PMCID: PMC2582494
- DOI: 10.1102/1470-7330.2008.9014
Item in Clipboard
Review
Critical questions in the imaging of colorectal hepatic metastases
Cancer Imaging.
.
Abstract
Aggressive treatment of patients with colorectal liver metastases can improve treatment outcome. In this paper, we review current management of patients with colorectal liver metastases and discuss the critical questions that the radiologist should consider when reviewing the imaging of these patients, so as to provide information that is important for formulating treatment strategies by the multidisciplinary management team.
Figures
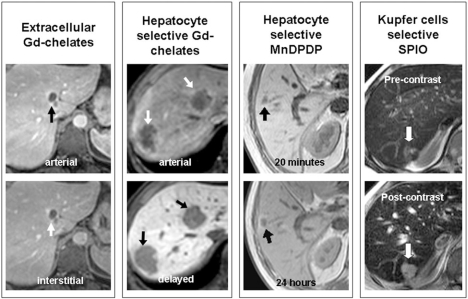
Illustrative examples of the appearances of colorectal liver metastases (arrows) after the administration of different contrast media. Left to right: using extracellular gadolinium chelates, metastases show rim enhancement in the arterial phase and appear hypointense to the liver in the portovenous phase on T1-weighted imaging. When a hepatocyte selective gadolinium contrast is used (e.g. Gd-EOB-DTPA), metastases show rim T1 enhancement in the arterial phase, but are most conspicuous as hypointense lesions in the delayed hepatocellular phase. Note the striking liver parenchymal enhancement with contrast washout from the intrahepatic vasculature in the delayed phase. Following MnDPDP contrast infusion, metastases typically appear as hypointense lesions against the enhancing liver parenchyma on T1-weighted imaging at 20 min. Rim enhancement is frequently observed around metastases at 24 h. The administration of SPIO contrast results in signal loss from the normal liver on T2* gradient echo imaging, facilitating the detection of the higher signal intensity metastases.
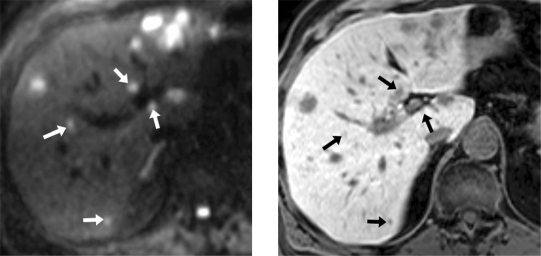
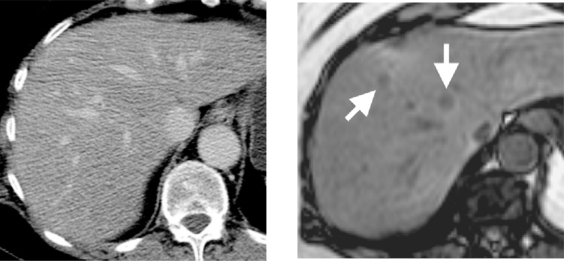
Diffusion-weighted MRI (DW-MRI) improves the detection of colorectal liver metastases. Left: delayed T1-weighted imaging after the administration of Gd-EOB-DTPA shows a number of hypointense metastases in the liver. Note, however, that the smaller metastases less than 1 cm in size (arrows) are easy to overlook, especially when they are located adjacent to intrahepatic vasculature, as they can mimic blood vessels. Right: DW-MRI performed using a b-value of 750 s/mm2 reveals both the larger and smaller (arrows) metastases as conspicuous high signal intensity lesions.
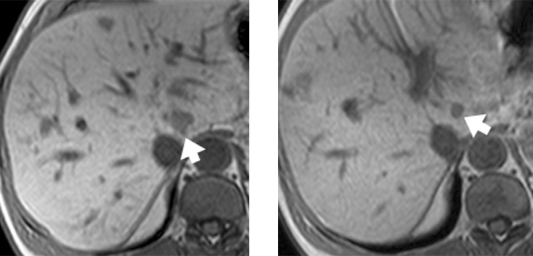
Neo-adjuvant chemotherapy with tumour regression. Pre-chemotherapy (left) and post-chemotherapy (right) T1-weighted MRI obtained at 20 min after the administration of MnDPDP contrast medium. Prior to neoadjuvant treatment, note the 2 cm hypointense metastasis (arrow) lying in close proximity to the intrahepatic inferior vena cava. Treatment with neoadjuvant chemotherapy resulted in downsizing of the metastasis to 1 cm in size with regression of tumour away from the inferior vena cava, thus facilitating surgical clearance.
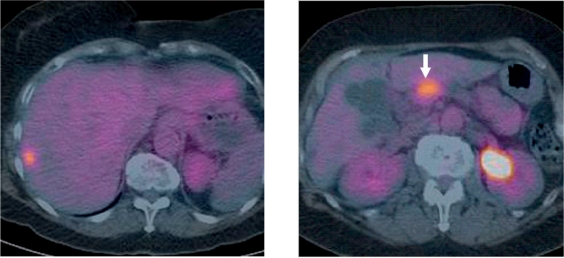
FDG-PET detects unsuspected extra-hepatic disease. Left: FDG-PET/CT of the liver demonstrated a solitary hypermetabolic liver metastasis in the right lobe of the liver. Right: FDG-PET/CT more inferiorly in the abdomen also showed increased tracer uptake in the neck of the pancreas which was confirmed to be an unsuspected pancreatic carcinoma, thus contraindicating curative surgical resection. Note that the low-density cysts in the liver showed no appreciable tracer uptake.
Diffuse liver steatosis can obscure liver metastases. Left: contrast-enhanced CT in the portovenous phase in a 45-year-old man shows diffuse low-density changes in the liver consistent with hepatic steatosis. Right: T1-weighted out-of-phase MR image shows signal loss in the liver parenchyma confirming fatty infiltration. However, two liver metastases (arrows) are also visible which are not seen at CT scanning.
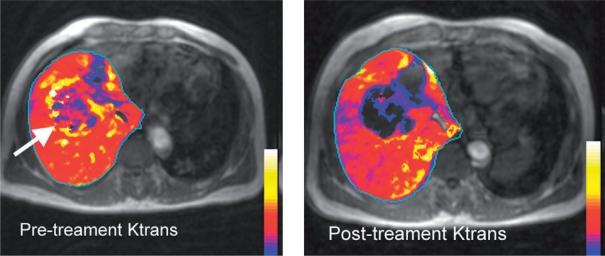
Maps of vascular parameter Ktrans obtained using DCE-MRI before and after vascular targeted therapy. These maps were created by overlaying the quantitative vascular parameter Ktrans (in colour) on the morphological T1-weighted images. Left: prior to treatment, the liver metastasis (arrow) showed an increase in Ktrans, particular at the tumour rim. Right: the Ktrans was substantially reduced at 14 days after the initiation of vascular targeted treatment.
Similar articles
-
Imaging and treatment of patients with colorectal liver metastases in the Netherlands: a survey.Neth J Med. 2006 May;64(5):147-51. Neth J Med. 2006. PMID: 16702613
-
Liver metastases from colorectal cancer: imaging with superparamagnetic iron oxide (SPIO)-enhanced MR imaging, computed tomography and positron emission tomography.Abdom Imaging. 2007 Sep-Oct;32(5):624-34. doi: 10.1007/s00261-007-9297-y. Abdom Imaging. 2007. PMID: 17710359
-
Imaging strategies before beginning treatment of colorectal liver metastases.Diagn Interv Imaging. 2014 May;95(5):505-12. doi: 10.1016/j.diii.2014.03.007. Epub 2014 Apr 30. Diagn Interv Imaging. 2014. PMID: 24794793 Review.
-
Gadoxetate disodium-enhanced magnetic resonance imaging versus contrast-enhanced 18F-fluorodeoxyglucose positron emission tomography/computed tomography for the detection of colorectal liver metastases.Invest Radiol. 2011 Sep;46(9):548-55. doi: 10.1097/RLI.0b013e31821a2163. Invest Radiol. 2011. PMID: 21577131
-
Current status of imaging and emerging techniques to evaluate liver metastases from colorectal carcinoma.Ann Surg. 2014 May;259(5):861-72. doi: 10.1097/SLA.0000000000000525. Ann Surg. 2014. PMID: 24509207 Review.
References
-
- Bipat S, van Leeuwen MS, Comans EF, et al. Colorectal liver metastases: CT, MR imaging, and PET for diagnosis – meta-analysis. Radiology. 2005;237:123–31. - PubMed
-
- Cromheecke M, de Jong KP, Hoekstra HJ. Current treatment for colorectal cancer metastatic to the liver. Eur J Surg Oncol. 1999;25:451–63. - PubMed
-
- Stangl R, Altendorf-Hofmann A, Charnley RM, Scheele J. Factors influencing the natural history of colorectal liver metastases. Lancet. 1994;343:1405–10. - PubMed
-
- Poston GJ. Surgical strategies for colorectal liver metastases. Surg Oncol. 2004;13:125–36. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical