

Smoking cessation interventions for hospitalized smokers: a systematic review
- PMID: 18852395
- PMCID: PMC4500120
- DOI: 10.1001/archinte.168.18.1950
Smoking cessation interventions for hospitalized smokers: a systematic review
Abstract
Background: A hospital admission provides an opportunity to help people stop smoking. Providing smoking cessation advice, counseling, or medication is now a quality-of-care measure for US hospitals. We assessed the effectiveness of smoking cessation interventions initiated during a hospital stay.
Methods: We searched the Cochrane Tobacco Addiction Review Group's register for randomized and quasirandomized controlled trials of smoking cessation interventions (behavioral counseling and/or pharmacotherapy) that began during hospitalization and had a minimum of 6 months of follow-up. Two authors independently extracted data from each article, with disagreements resolved by consensus.
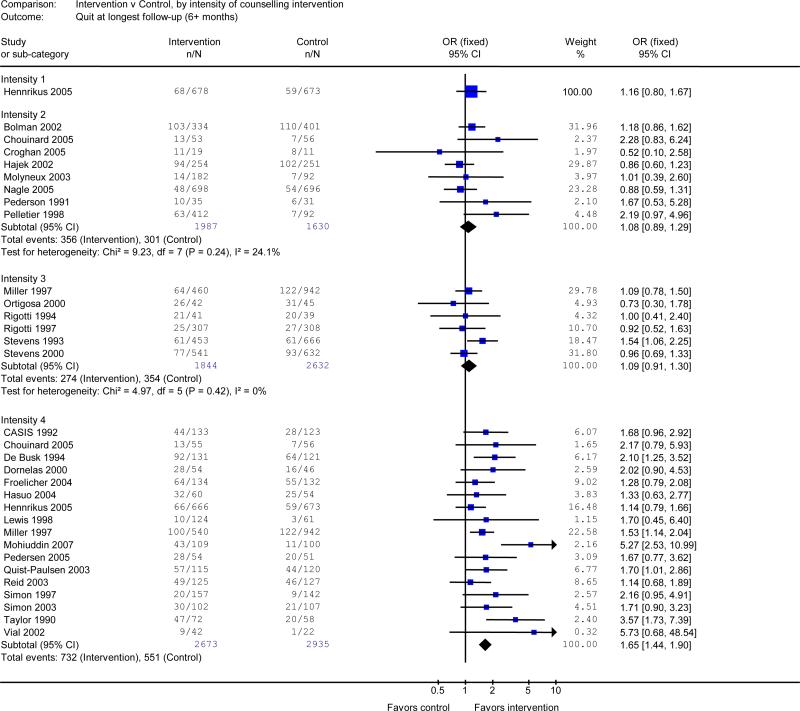
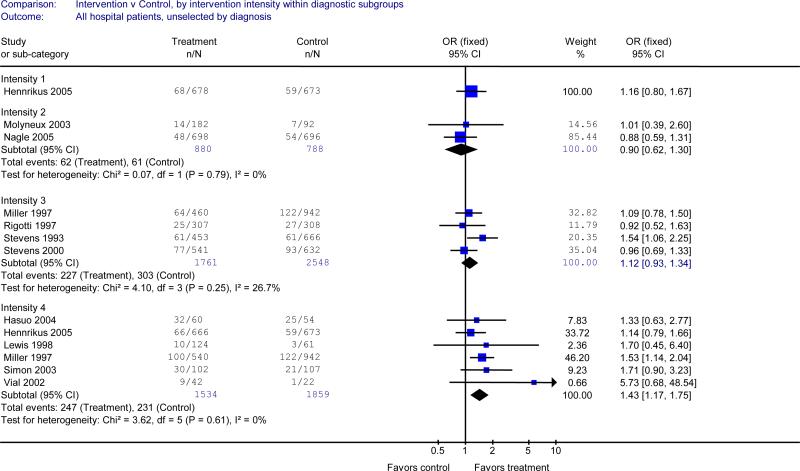
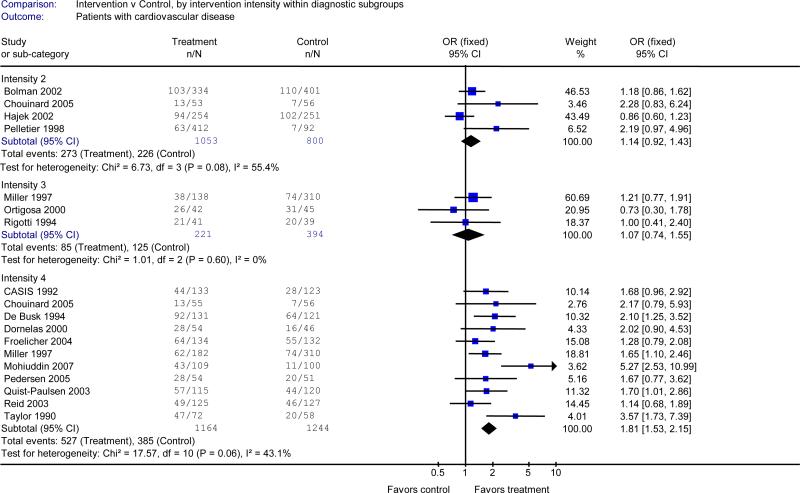
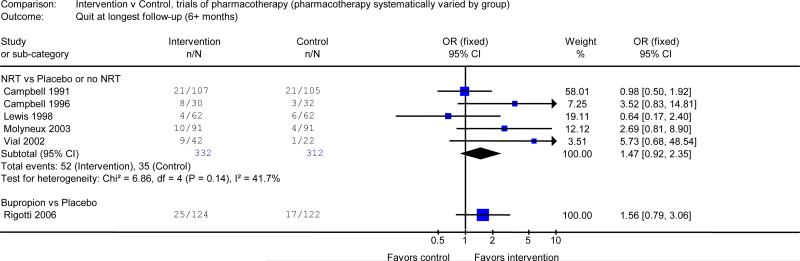
Results: Thirty-three trials met inclusion criteria. Smoking counseling that began during hospitalization and included supportive contacts for more than 1 month after discharge increased smoking cessation rates at 6 to 12 months (pooled odds ratio [OR], 1.65; 95% confidence interval [CI], 1.44-1.90). No benefit was found for interventions with less postdischarge contact. Counseling was effective when offered to all hospitalized smokers and to the subset admitted for cardiovascular disease. Adding nicotine replacement therapy to counseling produced a trend toward efficacy over counseling alone (OR, 1.47; 95% CI, 0.92-2.35). One study added bupropion hydrochloride to counseling, which had a nonsignificant result (OR, 1.56; 95% CI, 0.79-3.06).
Conclusions: Offering smoking cessation counseling to all hospitalized smokers is effective as long as supportive contacts continue for more than 1 month after discharge. Adding nicotine replacement therapy to counseling may further increase smoking cessation rates and should be offered when clinically indicated, especially to hospitalized smokers with nicotine withdrawal symptoms.
Figures
Comment in
-
Live fast, die young, leave a good-looking corpse.Arch Intern Med. 2008 Oct 13;168(18):1946-7. doi: 10.1001/archinte.168.18.1946. Arch Intern Med. 2008. PMID: 18852393 No abstract available.
References
-
- U.S. Department of Health and Human Services . The health consequences of smoking: A report of the surgeon general. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; Atlanta, GA: 2004.
-
- U.S. Department of Health and Human Services . Reducing tobacco use: A report of the surgeon general. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; Atlanta, GA: 2000.
-
- Longo DR, Brownson RC, Kruse RL. Smoking bans in US hospitals. results of a national survey. JAMA. 1995;274:488–491. - PubMed
-
- Joint Commission on Accreditation of Healthcare Organizations . A comprehensive review of development and testing for national implementation of hospital core measures. [September, 2007]. Available at: http://www.jointcommission.org/NR/rdonlyres/48DFC95A-9C05-4A44-AB05-1769....
-
- U.S. Department of Health and Human Services [September 6, 2007];Hospital compare- a quality tool for adults, including people with medicare. Available at: http://www.hospitalcompare.hhs.gov/Hospital.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
