

Case Reports
doi: 10.3174/ajnr.A1311.
Epub 2008 Oct 14.
Reversible encephalopathy after cardiac transplantation: histologic evidence of endothelial activation, T-cell specific trafficking, and vascular endothelial growth factor expression
Affiliations
- PMID: 18854444
- PMCID: PMC4526311
- DOI: 10.3174/ajnr.A1311
Item in Clipboard
Case Reports
Reversible encephalopathy after cardiac transplantation: histologic evidence of endothelial activation, T-cell specific trafficking, and vascular endothelial growth factor expression
AJNR Am J Neuroradiol.
2009 Mar.
Abstract
Reversible encephalopathy after transplantation is well recognized. The condition is commonly thought to be related to immune suppression, and a characteristic brain imaging pattern is typically recognized with vasogenic edema in the parietal and occipital regions, typically termed posterior reversible encephalopathy syndrome (PRES). We report the case of a patient with reversible encephalopathy after cardiac transplantation with brain biopsy evidence of endothelial activation, selective intravascular/perivascular T-cell trafficking, and VEGF expression in astrocytes, neurons, and the endothelium.
Figures

MR imaging studies of reversible encephalopathy. A, Axial MR fluid-attenuated inversion recovery image obtained at toxicity demonstrates vasogenic edema in the frontal lobes bilaterally (arrows). Minor small-vessel disease changes were also present (arrowhead). Diffusion sequence demonstrated T2 shinethrough, but true restricted diffusion was not present. B, Axial MR fluid-attenuated inversion recovery image obtained 1 month after right frontal lobe biopsy demonstrates near-complete resolution of the edema in the left frontal lobe (large arrow). Postbiopsy changes are present in the right frontal lobe (small arrows) with resolution of the previously present vasogenic edema deep to the biopsy changes. Residual small-vessel disease changes are again noted (arrowhead).

Early microscopic pathologic features of reversible encephalopathy, hematoxylin-eosin stain. A, Hematoxylin- eosin–stained sections showed many small blood vessels with reactive endothelial cells (black arrow) in the white matter demonstrating cellular and nuclear enlargement as well as mild interstitial edema (white arrow). Some vessels appeared nonreactive and are visible as a comparison (arrowhead). No vasculitis, demyelination, or axonal swelling was seen. Some scattered erythrocytes are present from the biopsy procedure, but no hemosiderin-laden macrophages were seen. B, These reactive blood vessels were also present in the gray matter, seen adjacent to a neuron (arrow), along with reactive astrocytes (arrowheads).

Early microscopic pathologic feature of reversible encephalopathy on immunohistochemical examination. A, CD45 (leukocyte common antigen) shows scattered lymphocytes in the intravascular (arrowhead) and perivascular (arrow) areas. The vessels identified by the arrows are shown in higher magnification in Figs B and C. B, Higher magnification of arrowhead in Fig 3A. Lymphocytes (T-cells) are regularly noted within the intravascular space (arrows) surrounded by endothelium (arrowhead). Other leukocytes (polymorphonuclear leukocytes, monocytes, macrophages) were not identified, suggesting selective T-lymphocyte adherence. C, Higher magnification of arrowhead in Fig 3A. Lymphocytes (T-cells) have traversed the endothelium (end point of the lymphocyte trafficking process) and are in the perivascular space (arrow). D, These lymphocytes were CD3-positive T-cells (arrow). No CD20-positive B-cells were present, and CD68 immunostaining identified only a modest number of activated microglia with no macrophages (not shown). Results of immunohistochemical and in situ hybridization studies were negative for toxoplasmosis, herpes simplex virus 1 and 2, Epstein-Barr virus, and JC virus (not shown). Results of tissue cultures were also negative.
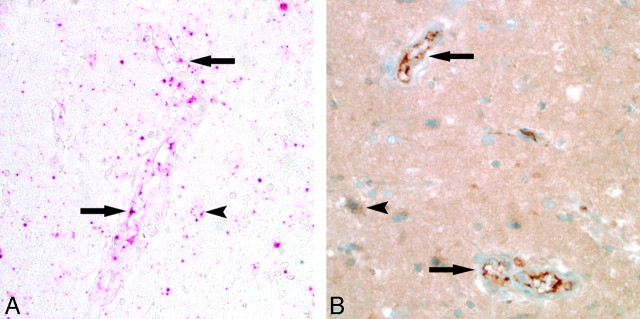
VEGF expression in reversible encephalopathy. A, In situ hybridization with a probe specific to VEGF messenger RNA showed robust transcription (red pigment) in the endothelium (arrows), astrocytes (arrowhead), and neurons. Results of biopsy of control brain tissue were negative (not shown). B, Immunohistochemical study for VEGF protein expression showed strong staining (deep brown pigment) in the brain tissue, including the endothelium (arrows), astrocytes (arrowhead), and neurons.
References
-
- Kilinc M, Benli S, Can U, et al. FK 506-induced fulminant leukoencephalopathy after kidney transplantation: case report. Transplant Proc 2002;34:1182–84 - PubMed
-
- Lanzino G, Cloft H, Hemstreet MK, et al. Reversible posterior leukoencephalopathy following organ transplantation. Description of two cases. Clin Neurol Neurosurg 1997;99:222–26 - PubMed
-
- Lavigne CM, Shrier DA, Ketkar M, et al. Tacrolimus leukoencephalopathy: a neuropathologic confirmation. Neurology 2004;63:1132–33 - PubMed
-
- Schiff D, Lopes MB. Neuropathological correlates of reversible posterior leukoencephalopathy. Neurocrit Care 2005;2:303–05 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical