

Peripapillary atrophy in Stargardt disease
- PMID: 18854780
- PMCID: PMC2743754
- DOI: 10.1097/IAE.0b013e31818a2c01
Peripapillary atrophy in Stargardt disease
Abstract
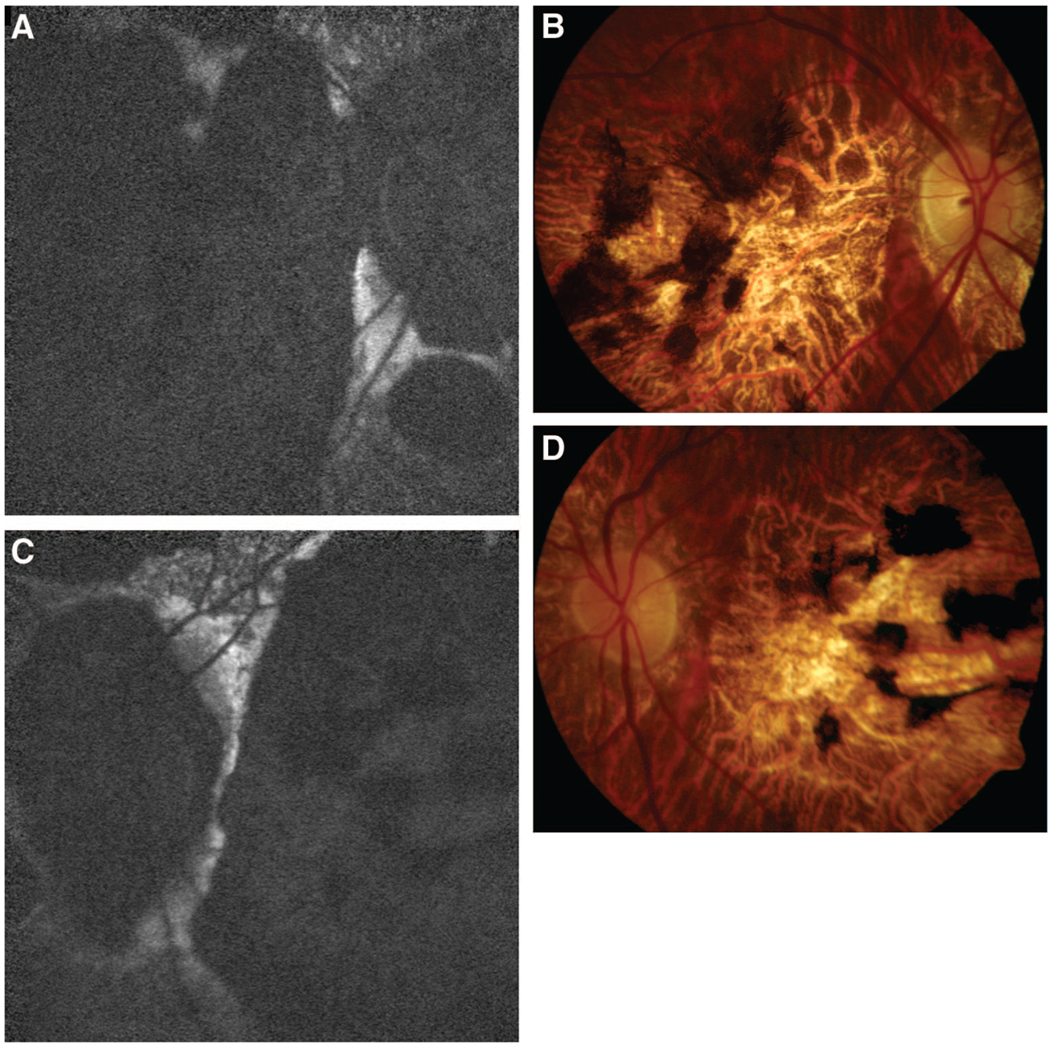
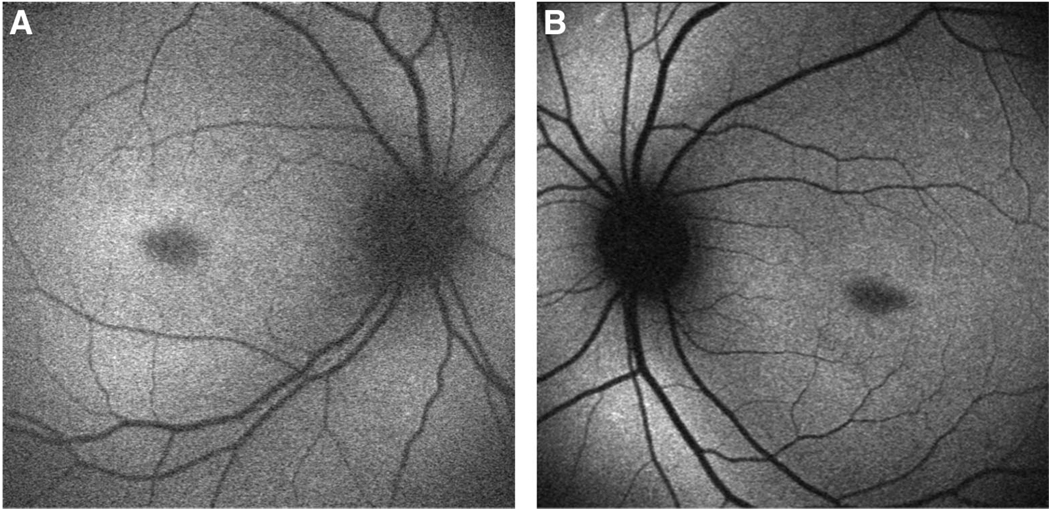
Objective: To demonstrate that Stargardt disease (STGD) can present with peripapillary atrophy.
Methods: Retrospective case series. The medical records of 150 consecutive patients (300 eyes) were reviewed retrospectively from a STGD database from January 1999 to May 2007 at Columbia University's Harkness Eye Institute. STGD patients demonstrating peripapillary atrophy were identified.
Results: Three of 150 cases of STGD (2.0%) demonstrated peripapillary atrophy. Case 1 revealed peripapillary and central atrophy with heterozygous ABCA4 mutations P1380L and IVS40 + 5G>A. Case 2 demonstrated atrophic fleck lesions involving the peripapillary region and central atrophy with homozygous ABCA4 mutations P1380L and P1380L. Case 3 revealed bilateral central atrophy and pisciform fleck atrophy involving the peripapillary, macular, and peripheral regions with ABCA4 mutations P1380L and R2030Q. Overall, ABCA4 mutation P1380L was noted in 13 cases (8.7%), IVS40 + 5G>A in 6 cases (4.0%), and R2030Q in 1 case (0.7%). The remaining cases shared one common STGD mutation with Case 1, 2, and 3 (P1380L or IVS40 + 5G>A) and demonstrated classic STGD findings of central atrophy and varying presence of peripheral flecks without peripapillary lesions.
Conclusion: STGD can present with peripapillary atrophy. This relatively uncommon phenotype may arise from specific combinations of STGD ABCA4 mutations rather than single mutations.
Figures



References
-
- Rotenstreich Y, Fishman GA, Anderson RJ. Visual acuity loss and clinical observations in a large series of patients with Stargardt disease. Ophthalmology. 2003;110:1151–1158. - PubMed
-
- Allikmets R, Singh N, Sun H, et al. A photoreceptor cell-specific ATP-binding transporter gene (ABCR) is mutated in recessive Stargardt macular dystrophy. Nat Genet. 1997;15:236–246. - PubMed
-
- Lois N, Halfyard AS, Bird AC, Holder GE, Fitzke FW. Fundus autofluorescence in Stargardt macular dystrophy-fundus flavimaculatus. Am J Ophthalmol. 2004;138:55–63. - PubMed
-
- Jaakson K, Zernant J, Kulm M, et al. Genotyping microarray (gene chip) for the ABCR (ABCA4) gene. Hum Mutat. 2003;22:395–403. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
