

Is PTEN loss associated with clinical outcome measures in human prostate cancer?
- PMID: 18854827
- PMCID: PMC2570524
- DOI: 10.1038/sj.bjc.6604680
Is PTEN loss associated with clinical outcome measures in human prostate cancer?
Abstract
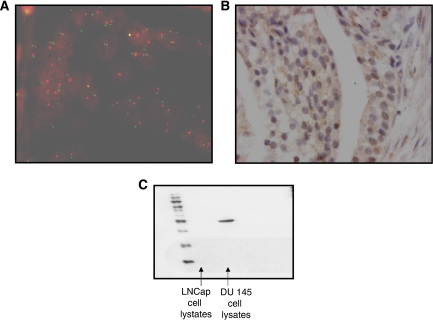
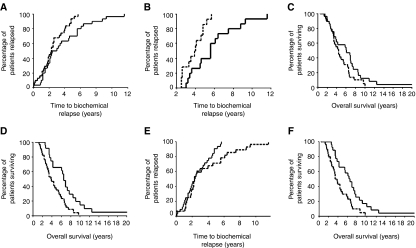
Inactivating PTEN mutations are commonly found in prostate cancer, resulting in an increased activation of Akt. In this study, we investigate the role of PTEN deletion and protein expression in the development of hormone-refractory prostate cancer using matched hormone-sensitive and hormone-refractory tumours. Fluorescent in situ hybridisation and immunohistochemistry was carried out to investigate PTEN gene deletion and PTEN protein expression in the transition from hormone-sensitive to hormone-refractory prostate cancer utilising 68 matched hormone sensitive and hormone-refractory tumour pairs (one before and one after hormone relapse). Heterogeneous PTEN gene deletion was observed in 23% of hormone sensitive tumours. This increased significantly to 52% in hormone-refractory tumours (P=0.044). PTEN protein expression was observed in the membrane, cytoplasm and the nucleus. In hormone sensitive tumours, low levels of cytoplasmic PTEN was independently associated with shorter time to relapse compared to high levels of PTEN (P=0.028, hazard ratio 0.51 (95%CI 0.27-0.93). Loss of PTEN expression in the nucleus of hormone sensitive tumours was independently associated with disease-specific survival (P=0.031, hazard ratio 0.52, 95%CI 0.29-0.95). The results from this study demonstrate a role for both cytoplasmic and nuclear PTEN in progression of prostate cancer to the hormone-refractory state.
Figures
References
-
- Burton JL, Oakley N, Anderson JB (2000) Recent advances in the histopathology and molecular biology of prostate cancer. BJU Int 85: 87–94 - PubMed
-
- Cancer Research UK web site (2004) Cancer Research UK web site. Cancer Stats. Mortality: UK. Available at http://www.cancerresearchuk.org
-
- Chung JH, Eng C (2005) Nuclear-cytoplasmic partitioning of phosphatase and tensin homologue deleted on chromosome 10 (PTEN) differentially regulates the cell cycle and apoptosis. Cancer Res 65: 8096–8100 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
