

Multiple giant cell lesions in patients with Noonan syndrome and cardio-facio-cutaneous syndrome
- PMID: 18854871
- PMCID: PMC2986220
- DOI: 10.1038/ejhg.2008.188
Multiple giant cell lesions in patients with Noonan syndrome and cardio-facio-cutaneous syndrome
Abstract
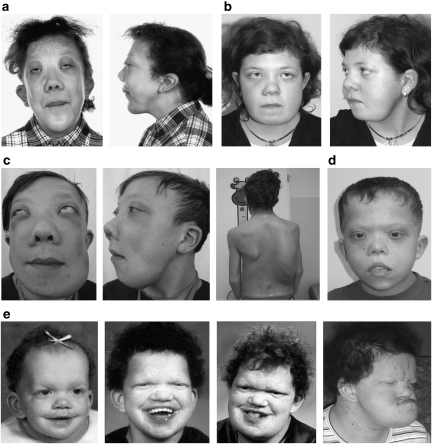
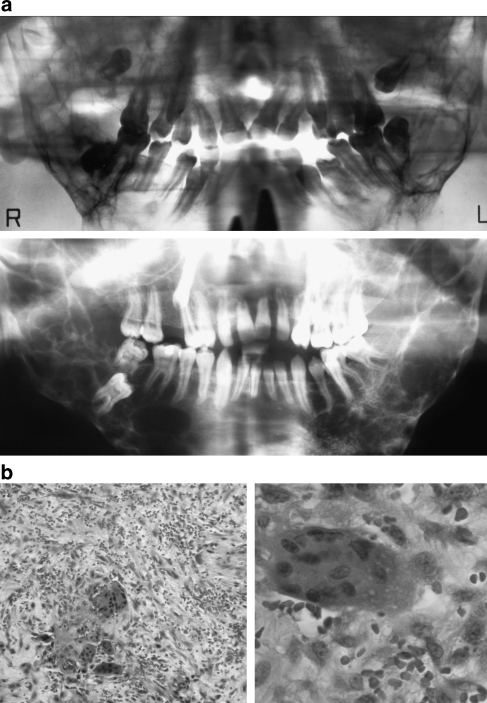
Noonan syndrome (NS) and cardio-facio-cutaneous syndrome (CFCS) are related developmental disorders caused by mutations in genes encoding various components of the RAS-MAPK signaling cascade. NS is associated with mutations in the genes PTPN11, SOS1, RAF1, or KRAS, whereas CFCS can be caused by mutations in BRAF, MEK1, MEK2, or KRAS. The NS phenotype is rarely accompanied by multiple giant cell lesions (MGCL) of the jaw (Noonan-like/MGCL syndrome (NL/MGCLS)). PTPN11 mutations are the only genetic abnormalities reported so far in some patients with NL/MGCLS and in one individual with LEOPARD syndrome and MGCL. In a cohort of 75 NS patients previously tested negative for mutations in PTPN11 and KRAS, we detected SOS1 mutations in 11 individuals, four of whom had MGCL. To explore further the relevance of aberrant RAS-MAPK signaling in syndromic MGCL, we analyzed the established genes causing CFCS in three subjects with MGCL associated with a phenotype fitting CFCS. Mutations in BRAF or MEK1 were identified in these patients. All mutations detected in these seven patients with syndromic MGCL had previously been described in NS or CFCS without apparent MGCL. This study demonstrates that MGCL may occur in NS and CFCS with various underlying genetic alterations and no obvious genotype-phenotype correlation. This suggests that dysregulation of the RAS-MAPK pathway represents the common and basic molecular event predisposing to giant cell lesion formation in patients with NS and CFCS rather than specific mutation effects.
Figures
References
-
- Noonan JA. Hypertelorism with Turner phenotype. A new syndrome with associated congenital heart disease. Am J Dis Child. 1968;116:373–380. - PubMed
-
- Tartaglia M, Mehler EL, Goldberg R, et al. Mutations in PTPN11, encoding the protein tyrosine phosphatase SHP-2, cause Noonan syndrome. Nat Genet. 2001;29:465–468. - PubMed
-
- Roberts AE, Araki T, Swanson KD, et al. Germline gain-of-function mutations in SOS1 cause Noonan syndrome. Nat Genet. 2007;39:70–74. - PubMed
-
- Tartaglia M, Pennacchio LA, Zhao C, et al. Gain-of-function SOS1 mutations cause a distinctive form of Noonan syndrome. Nat Genet. 2007;39:75–79. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
