

Osteosarcoma of the pelvis: outcome analysis of surgical treatment
- PMID: 18855090
- PMCID: PMC2628496
- DOI: 10.1007/s11999-008-0495-x
Osteosarcoma of the pelvis: outcome analysis of surgical treatment
Abstract
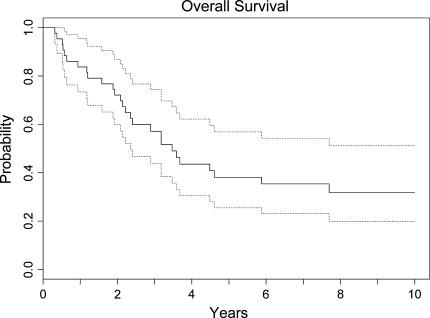
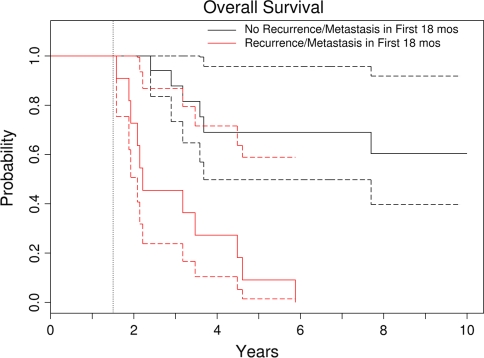
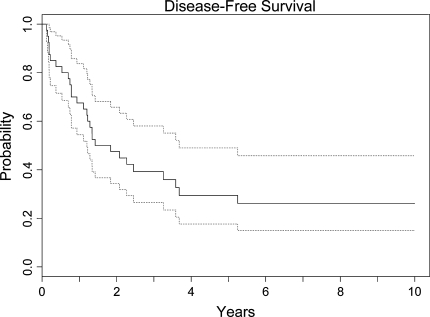
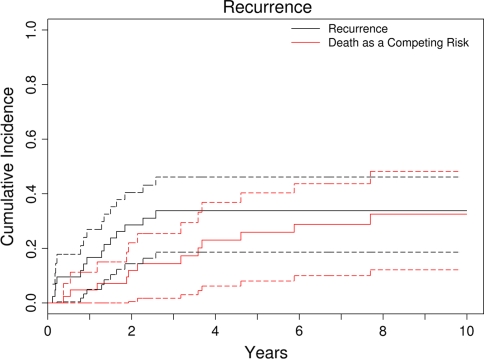
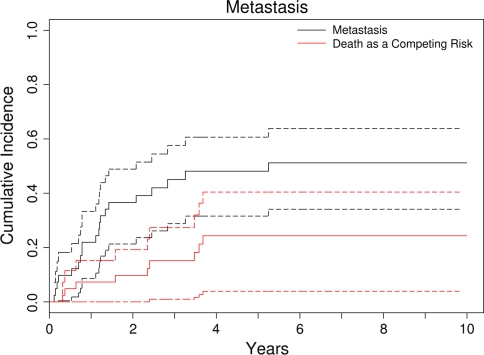
Risk factors to explain the poor survival of patients with osteosarcoma of the pelvis are poorly understood. Therefore, we attempted to identify factors affecting survival and development of local recurrence and metastasis. We retrospectively reviewed 43 patients who had high-grade pelvic tumors and were treated surgically. Twenty lesions were chondroblastic, 10 fibroblastic, 11 osteoblastic, and one each was giant cell-rich and small cell osteosarcomas. At a median of 3.5 years (range, 0.3-21 years) postoperatively, 13 patients were alive with no evidence of disease. The overall and disease-free 5-year survival rates were 38% and 29%, respectively, at 5 years. Anatomic location, tumor size, and margin predicted survival. Fifteen patients (35%) had local recurrence. The 5-year cumulative incidence of recurrence with death as a competing risk factor was 34%. Location in the ilium and size of the tumor predicted local recurrence. Twenty-one (49%) of 43 patients had metastases develop. The cumulative incidence of metastasis with death as a competing risk factor was 48% at 5 years. Six patients who presented with metastasis had a worse survival than patients who had no evidence of metastasis at presentation (2-year survival, 33% versus 76%). If distant metastasis is diagnosed subsequent to primary treatment, aggressive therapy may be justified.
Level of evidence: Level II, prognostic study. See the Guidelines for Authors for a complete description of levels of evidence.
Figures
References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1200/JCO.20.3.776', 'is_inner': False, 'url': 'https://doi.org/10.1200/jco.20.3.776'}, {'type': 'PubMed', 'value': '11821461', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/11821461/'}]}
- Bielack SS, Kempf-Bielack B, Delling G, Exner GU, Flege S, Helmke K, Kotz R, Salzer-Kuntschik M, Werner M, Winkelmann W, Zoubek A, Jurgens H, Winkler K. Prognostic factors in high-grade osteosarcoma of the extremities or trunk: an analysis of 1,702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols. J Clin Oncol. 2002;20:776–790. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1002/mpo.2950240103', 'is_inner': False, 'url': 'https://doi.org/10.1002/mpo.2950240103'}, {'type': 'PubMed', 'value': '7968796', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/7968796/'}]}
- Bielack SS, Wulff B, Delling G, Gobel U, Kotz R, Ritter J, Winkler K. Osteosarcoma of the trunk treated by multimodal therapy: experience of the Cooperative Osteosarcoma study group (COSS). Med Pediatr Oncol. 1995;24:6–12. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '1652313', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/1652313/'}]}
- Campanacci M, Ruggieri P. Osteosarcoma. Bull Hosp Jt Dis Orthop Inst. 1991;51:1–11. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1016/j.ejso.2003.12.004', 'is_inner': False, 'url': 'https://doi.org/10.1016/j.ejso.2003.12.004'}, {'type': 'PubMed', 'value': '15028318', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/15028318/'}]}
- Donati D, Giacomini S, Gozzi E, Ferrari S, Sangiorgi L, Tienghi A, DeGroot H, Bertoni F, Bacchini P, Bacci G, Mercuri M. Osteosarcoma of the pelvis. Eur J Surg Oncol. 2004;30:332–340. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '701308', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/701308/'}]}
- Enneking WF, Dunham WK. Resection and reconstruction for primary neoplasms involving the innominate bone. J Bone Joint Surg Am. 1978;60:731–746. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
