

Vitamin K supplementation in postmenopausal women with osteopenia (ECKO trial): a randomized controlled trial
- PMID: 18922041
- PMCID: PMC2566998
- DOI: 10.1371/journal.pmed.0050196
Vitamin K supplementation in postmenopausal women with osteopenia (ECKO trial): a randomized controlled trial
Erratum in
- PLoS Med. 2008 Dec;5(12):e247
Abstract
Background: Vitamin K has been widely promoted as a supplement for decreasing bone loss in postmenopausal women, but the long-term benefits and potential harms are unknown. This study was conducted to determine whether daily high-dose vitamin K1 supplementation safely reduces bone loss, bone turnover, and fractures.
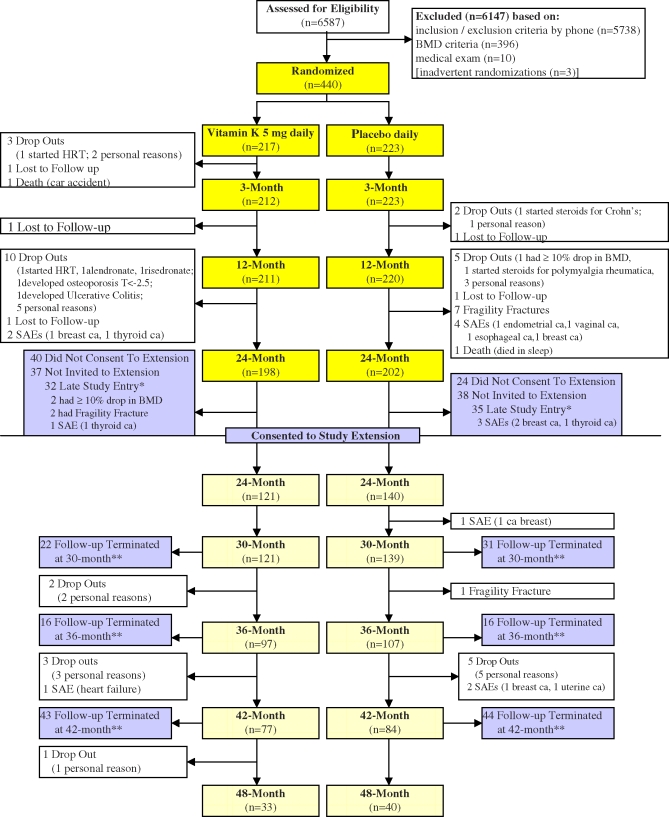
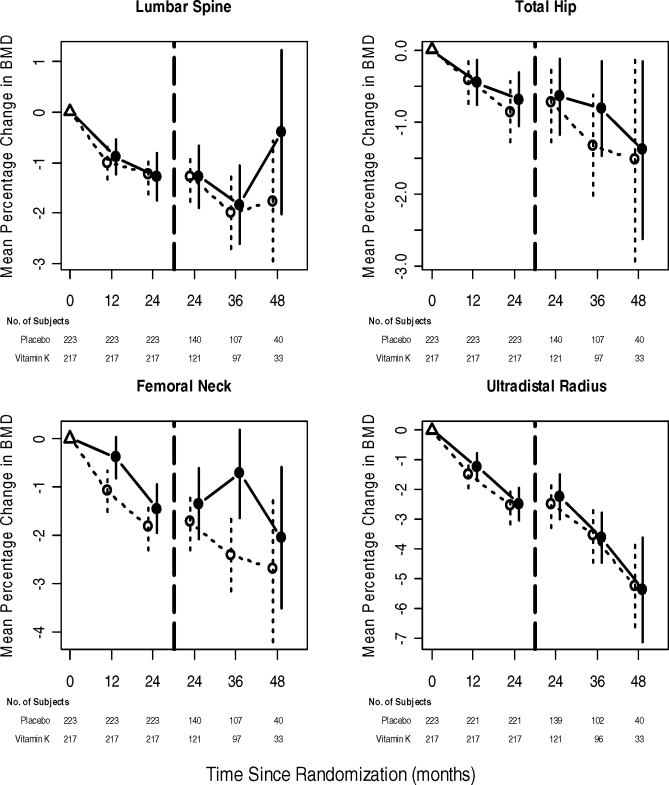
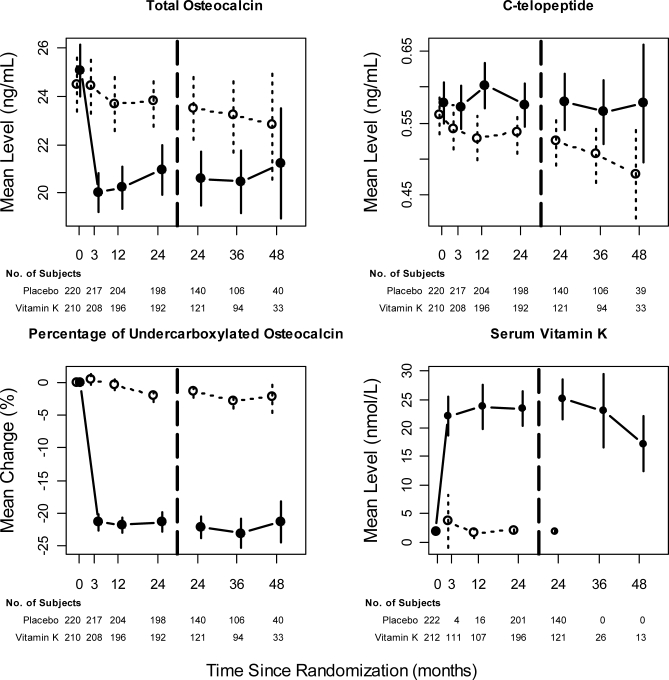
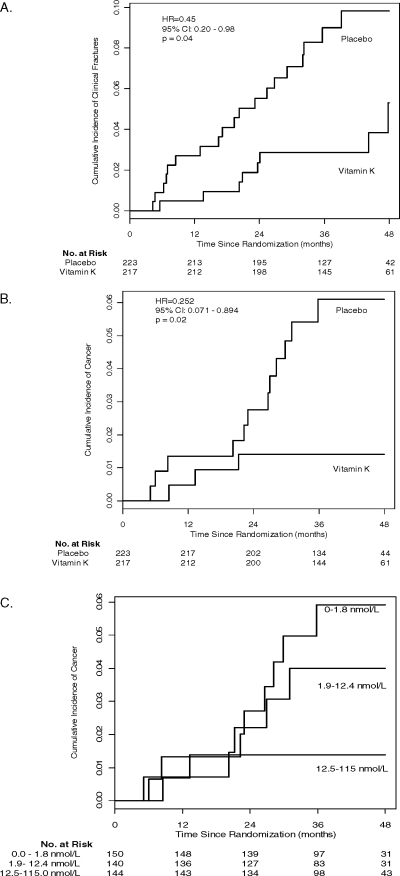
Methods and findings: This single-center study was designed as a 2-y randomized, placebo-controlled, double-blind trial, extended for earlier participants for up to an additional 2 y because of interest in long-term safety and fractures. A total of 440 postmenopausal women with osteopenia were randomized to either 5 mg of vitamin K1 or placebo daily. Primary outcomes were changes in BMD at the lumbar spine and total hip at 2 y. Secondary outcomes included changes in BMD at other sites and other time points, bone turnover markers, height, fractures, adverse effects, and health-related quality of life. This study has a power of 90% to detect 3% differences in BMD between the two groups. The women in this study were vitamin D replete, with a mean serum 25-hydroxyvitamin D level of 77 nmol/l at baseline. Over 2 y, BMD decreased by -1.28% and -1.22% (p = 0.84) (difference of -0.06%; 95% confidence interval [CI] -0.67% to 0.54%) at the lumbar spine and -0.69% and -0.88% (p = 0.51) (difference of 0.19%; 95% CI -0.37% to 0.75%) at the total hip in the vitamin K and placebo groups, respectively. There were no significant differences in changes in BMD at any site between the two groups over the 2- to 4-y period. Daily vitamin K1 supplementation increased serum vitamin K1 levels by 10-fold, and decreased the percentage of undercarboxylated osteocalcin and total osteocalcin levels (bone formation marker). However, C-telopeptide levels (bone resorption marker) were not significantly different between the two groups. Fewer women in the vitamin K group had clinical fractures (nine versus 20, p = 0.04) and fewer had cancers (three versus 12, p = 0.02). Vitamin K supplements were well-tolerated over the 4-y period. There were no significant differences in adverse effects or health-related quality of life between the two groups. The study was not powered to examine fractures or cancers, and their numbers were small.
Conclusions: Daily 5 mg of vitamin K1 supplementation for 2 to 4 y does not protect against age-related decline in BMD, but may protect against fractures and cancers in postmenopausal women with osteopenia. More studies are needed to further examine the effect of vitamin K on fractures and cancers.
Trial registration: ClinicalTrials.gov (#NCT00150969) and Current Controlled Trials (#ISRCTN61708241).
Conflict of interest statement
Figures
References
-
- Mercola J, Droege R. 10 Important facts about vitamin K that you need to know. 2004. Available: http://www.mercola.com/forms/vitamin_k2.htm. Accessed 24 March 2004.
-
- Thomson Healthcare. PDRhealth on Vitamin K. 2007. Available: http://www.pdrhealth.com/drugs/altmed/altmed-mono.aspx?contentFileName=a.... Accessed 12 July 2007.
-
- Booth SL, Broe KE, Gagnon DR, Tucker KL, Hannan MT, et al. Vitamin K intake and bone mineral density in women and men. Am J Clin Nutr. 2003;77:512–516. - PubMed
-
- Booth SL, Broe KE, Peterson JW, Cheng DM, Dawson-Hughes B, et al. Associations between vitamin K biochemical measures and bone mineral density in men and women. J Clin Endocrin Metab. 2004;89:4904–4909. - PubMed
-
- Feskanich D, Weber P, Willett WC, Rockett H, Booth SL, et al. Vitamin K intake and hip fractures in women: a prospective study. Am J Clin Nutr. 1999;69:74–79. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
