

Physical activity and hemodynamic reactivity in chronic kidney disease
- PMID: 18922983
- PMCID: PMC2572287
- DOI: 10.2215/CJN.02920608
Physical activity and hemodynamic reactivity in chronic kidney disease
Abstract
Background and objectives: Patients with chronic kidney disease (CKD) have an elevated cardiovascular risk. This study was designed to understand better the presence and strength of the relationship between physical activity and BP and to explore determinants of hemodynamic reactivity.
Design, setting, participants, & measurements: Twenty-four patients with CKD (mean age 69.5 yr; 3.1 antihypertensive drugs; estimated GFR 47 ml/min per 1.73 m(2), albumin/creatinine ratio 403 mg/g) were studied on three occasions during a 6-wk period with 24-h ambulatory BP monitoring and simultaneous activity monitoring with wrist actigraphy.
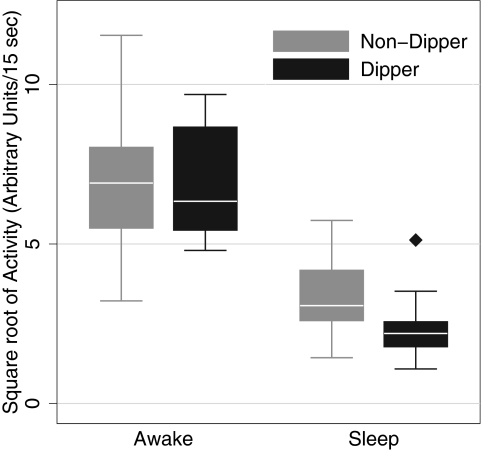
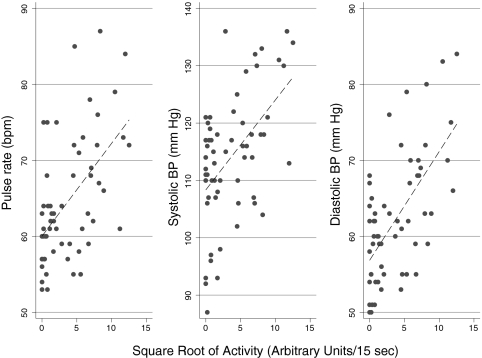
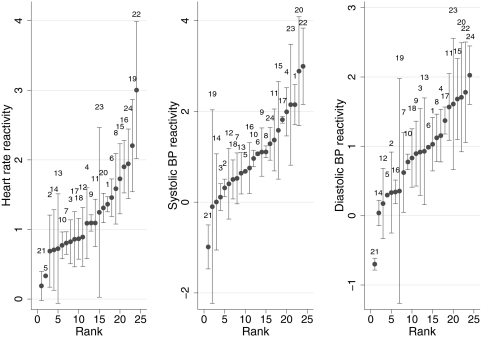
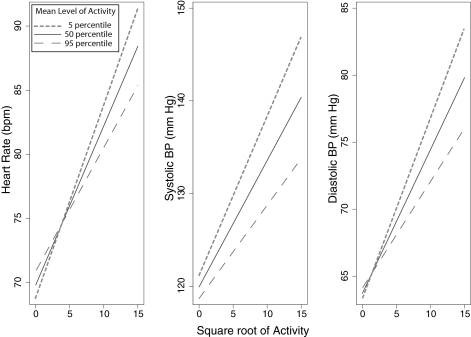
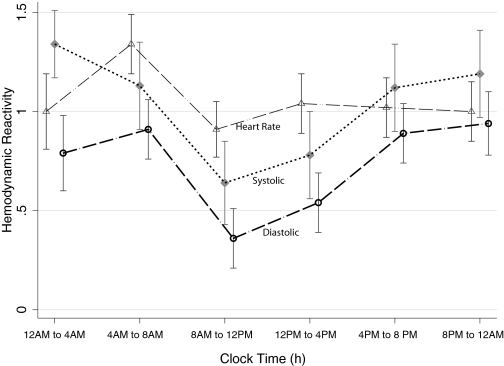
Results: Nondippers were found have a greater level of sleep activity compared with dippers, although the awake activity level was similar (7.06 versus 6.73) between groups (P = 0.042 for interaction). In 3587 BP activity pairs, hemodynamic reactivity was variable between individuals (systolic BP reactivity 1.06 [SD 10.50]; diastolic BP reactivity 0.89 [SD 7.80] heart rate reactivity 1.18 [SD 11.00]); those who were more sedentary had a greater increment in systolic BP compared with those who were less sedentary. Antihypertensive drugs blunted hemodynamic reactivity. Hemodynamic reactivity was greatest between 12 a.m. and 8 a.m., making this a vulnerable period for cardiovascular events.
Conclusions: Greater hemodynamic reactivity in sedentary people with CKD offers a possible and thus far unrecognized mechanism of cardiovascular damage. Besides reducing BP, antihypertensive drugs reduce hemodynamic reactivity, which offers another plausible mechanism of cardiovascular protection with their use.
Figures
References
-
- Clark LA, Denby L, Pregibon D, Harshfield GA, Pickering TG, Blank S, Laragh JH: A quantitative analysis of the effects of activity and time of day on the diurnal variations of blood pressure. J Chronic Dis 40: 671–681, 1987 - PubMed
-
- Kuwajima I, Hamamatsu A, Suzuki Y, Kuramoto K: The relationship between ambulatory blood pressure and physical activity in young and older shiftworkers: A quantitative assessment of physical activity using a microcomputer with acceleration sensor. Jpn Heart J 34: 279–289, 1993 - PubMed
-
- Van Egeren LF: Monitoring activity and blood pressure. J Hypertens Suppl 9: S25–S27, 1991 - PubMed
-
- Stewart MJ, Brown H, Padfield PL: Can simultaneous ambulatory blood pressure and activity monitoring improve the definition of blood pressure? Am J Hypertens 6: 174S–178S, 1993 - PubMed
-
- Gretler DD, Carlson GF, Montano AV, Murphy MB: Diurnal blood pressure variability and physical activity measured electronically and by diary. Am J Hypertens 6: 127–133, 1993 - PubMed
