

Chronic kidney disease after hematopoietic cell transplantation: a systematic review
- PMID: 18925905
- PMCID: PMC3564956
- DOI: 10.1111/j.1600-6143.2008.02408.x
Chronic kidney disease after hematopoietic cell transplantation: a systematic review
Erratum in
- Am J Transplant. 2009 Apr;9(4):865. Kambay, M [corrected to Kanbay, M]
Abstract
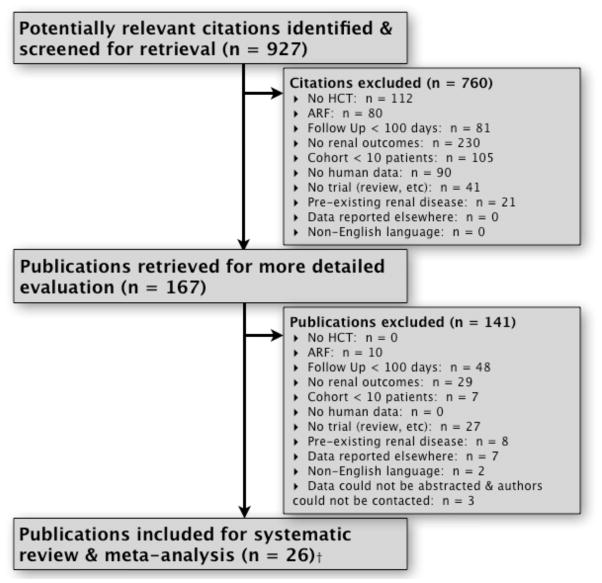
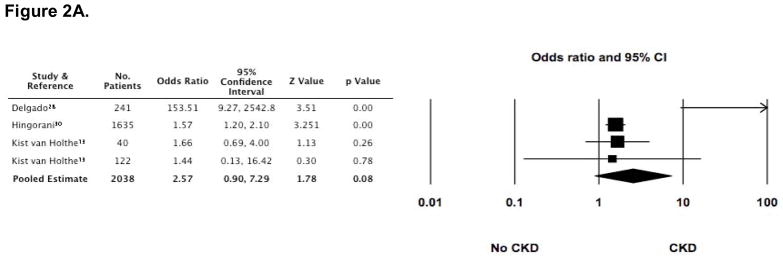
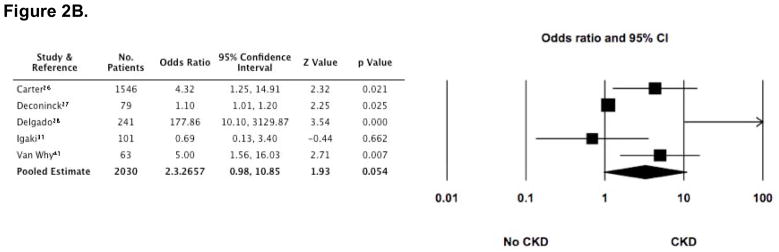
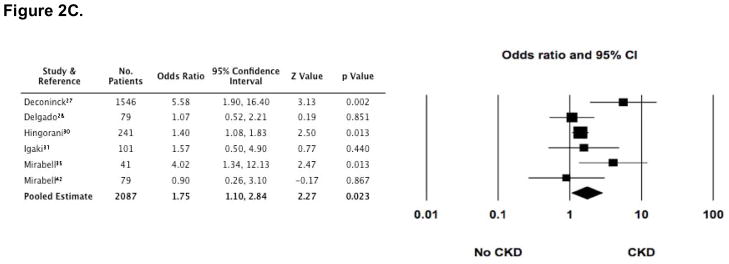
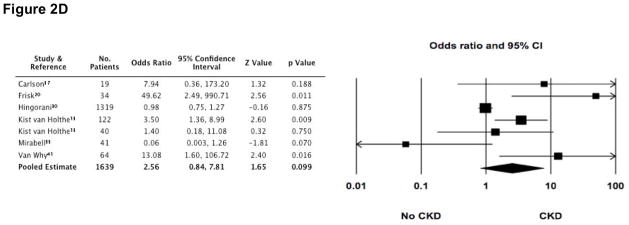
Advances in hematopoietic cell transplantation (HCT) have broadened its indications for use and resulted in more long-term HCT survivors. Some survivors develop chronic kidney disease (CKD); however, the incidence and risk factors are unclear. We performed a systematic review of studies identified from databases (MEDLINE, EMBASE, Science Citation Index), conference abstracts and reference lists from selected manuscripts. From 927 manuscripts, 28 patient cohorts were identified in which 9317 adults and children underwent HCT and 7317 (79%) survived to at least 100 days, permitting inclusion of 5337 (73% of survivors) in quantitative analyses. Although definitions and measurements varied widely, approximately 16.6% of HCT patients developed CKD and estimated glomerular filtration rate (eGFR in mL/min/1.73 m(2)) decreased by 24.5 after 24 months. This decrease was greater amongst patients undergoing allogeneic HCT (DeltaeGFR = -40.0 versus -18.6 for autologous transplants). Several commonly reported risk factors for CKD were investigated, including acute renal failure, total body irradiation, graft versus host disease and long-term cyclosporine use. In conclusion, CKD following HCT is likely to be common; however, prospective studies with uniform definitions of CKD and risk factors are needed to confirm these findings and better define the underlying mechanisms to promote therapies that prevent this complication.
Conflict of interest statement
Conflict-of-Interest disclosure: The authors declare no competing financial interests.
Figures
Similar articles
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Polyclonal and monoclonal antibodies for treating acute rejection episodes in kidney transplant recipients.Cochrane Database Syst Rev. 2017 Jul 20;7(7):CD004756. doi: 10.1002/14651858.CD004756.pub4. Cochrane Database Syst Rev. 2017. PMID: 28731207 Free PMC article.
-
Transfusion thresholds for guiding red blood cell transfusion.Cochrane Database Syst Rev. 2021 Dec 21;12(12):CD002042. doi: 10.1002/14651858.CD002042.pub5. Cochrane Database Syst Rev. 2021. PMID: 34932836 Free PMC article.
-
Interventions for promoting habitual exercise in people living with and beyond cancer.Cochrane Database Syst Rev. 2018 Sep 19;9(9):CD010192. doi: 10.1002/14651858.CD010192.pub3. Cochrane Database Syst Rev. 2018. PMID: 30229557 Free PMC article.
-
Nivolumab for adults with Hodgkin's lymphoma (a rapid review using the software RobotReviewer).Cochrane Database Syst Rev. 2018 Jul 12;7(7):CD012556. doi: 10.1002/14651858.CD012556.pub2. Cochrane Database Syst Rev. 2018. PMID: 30001476 Free PMC article.
Cited by
-
Chronic kidney disease, survival and graft-versus-host-disease-free/relapse-free survival in recipients of allogeneic hematopoietic stem cell transplant.Clin Kidney J. 2022 Apr 7;15(8):1583-1592. doi: 10.1093/ckj/sfac091. eCollection 2022 Aug. Clin Kidney J. 2022. PMID: 35892015 Free PMC article.
-
An Overview of Kidney Disease Following Hematopoietic Cell Transplantation.Intern Med. 2018 Jun 1;57(11):1503-1508. doi: 10.2169/internalmedicine.9838-17. Epub 2018 Jan 11. Intern Med. 2018. PMID: 29321440 Free PMC article. Review.
-
Chronic kidney disease after hematopoietic stem cell transplantation.Semin Nephrol. 2010 Nov;30(6):627-34. doi: 10.1016/j.semnephrol.2010.09.010. Semin Nephrol. 2010. PMID: 21146127 Free PMC article. Review.
-
Mini-review of kidney disease following hematopoietic stem cell transplant .Clin Nephrol. 2018 Jun;89(6):389-402. doi: 10.5414/CN109276. Clin Nephrol. 2018. PMID: 29578399 Free PMC article. Review.
-
Symptomatic BK Virus Infection Is Associated With Kidney Function Decline and Poor Overall Survival in Allogeneic Hematopoietic Stem Cell Recipients.Am J Transplant. 2016 May;16(5):1492-502. doi: 10.1111/ajt.13635. Epub 2016 Mar 2. Am J Transplant. 2016. PMID: 26608093 Free PMC article.
References
-
- Current Use and Outcome of Hematopoietic Stem Cell Transplantation. CIBMTR; 2007. [Accessed January 14, 2008]. < http://campus.mcw.edu/AngelUploads/Content/CS_IBMTR2/_assoc/ECCBED0AF0A4...>.
-
- Copelan EA. Hematopoietic stem-cell transplantation. N Engl J Med. 2006;354:1813–1826. - PubMed
-
- Yee GC, McGuire TR, St Pierre BA, et al. Minimal risk of chronic renal dysfunction in marrow transplant recipients treated with cyclosporine for 6 months. Bone Marrow Transplant. 1989;4:691–694. - PubMed
-
- Weiss AS, Sandmaier BM, Storer B, Storb R, McSweeney PA, Parikh CR. Chronic kidney disease following non-myeloablative hematopoietic cell transplantation. Am J Transplant. 2006;6:89–94. - PubMed
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351:1296–1305. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
